
EVALUATION OF PHARYNGEAL AIRWAY AND HYOID BONE POSITION ACCORDING TO DIFFERENT GROWTH-DEVELOPMENT PERIODS
Elif Albayrak 1![]()
![]() , Muhammed
Hilmi Büyükçavuş 2
, Muhammed
Hilmi Büyükçavuş 2![]()
![]()
1 DDS, PhD, Private Practice, Department of Orthodontics, Antalya, Turkey
2 DDS, Associate Professor, Süleyman Demirel University, Faculty of
Dentistry, Department of Orthodontics, Isparta, Turkey
|
|
|
ABSTRACT |
|
|
Background: The aim of this study was to evaluate the pharyngeal airway and hyoid measurements according to gender and pre-peak, peak and post-peak growth-development stages. Method: In our study were included 531 people. The classification of the patients according to the pubertal growth attack periods in the grouping according to the growth-development period was determined from the lateral cephalometric films taken at the beginning of the treatment. The pharyngeal airway and hyoid measurements were compared according to three different growth-development periods. SPSS program was used for data analysis. Results: A statistical relationship was observed between growth-development periods, gender, and chronological age (p<0.05). A statistically significant difference was found in the majority (86%) of pharyngeal airway dimensions and hyoid measurements in all three groups (p<0.05). Conclusions: With
age and as the growth-development periods progress, the dimensions of the
pharyngeal airway increase, and the hyoid bone moves downwards. |
|||
|
Received 09 April 2022 Accepted 15 May 2022 Published 31 May 2022 Corresponding Author Elif Albayrak,
DOI 10.29121/granthaalayah.v10.i4.2022.4590 Funding: The authors of
this study declare that they self- funded the current study. Copyright: © 2022 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Pharyngeal Airway, Hyoid Bone, Cervical Vertebra,
Cephalometry |
|||
1. INTRODUCTION
Vertebrae, cranial base, jaws, nasal septum, and hyoid bone, which form the skeletal support of the airway, also play a role in growth Schendel et al. (2012). Since the posterior cranial base forms, the upper borders of the pharynx, the growth of this structure affects the growth of the pharynx. The growth of the sphenoid wings and the forward dragging of the palate cause the nasopharynx to expand. When the pharyngeal depth is measured as the distance from the posterior nasal spine to the basion, it is quite limited, and a small increase (9%) has been reported Tourné (1991). The main growth direction of the pharynx is vertical, and this is statistically significant with the age of the patient and continues until adulthood Martin et al. (2011). Vertical enlargement and downward rotation of the hard palate in sphenooccipital synchondrosis increases the height of the nasopharynx by approximately 38% and accounts for most of the increase in nasopharyngeal capacity Tourné (1991). Pharyngeal growth is transversely affected by changes in the medial pterygoid laminae.
Bergland reported in his study in 1963 that the increase in width started after the age of 6 and the increase in width accelerated during adolescence Aloufi et al. (2012). In a study in the literature, they stated that the thickness of the soft tissue in the posterior nasopharyngeal wall is maximum at the age of 5 years and decreases until the age of 10, and it increases slightly between the ages of 10-11 and continues to decrease. In the study examining the growth of soft tissues in the oropharyngeal region, they stated that the posterior pharyngeal wall measurements increased between the ages of 6-9 and 12-15, and little change occurred between the ages of 9-12 and 12-15 years. They also reported that the distance between the anterior border of the atlas and the PNS remained constant after the age of 12. This situation: shows that there is no increase in size after pubertal growth spurt in the pharynx bones Taylor et al. (1996).
The hyoid bone, which plays an important role in the realization of tongue functions, providing cranial balance and straightening the head posture; it is not connected to any bone in the skull skeleton, but is connected to the surrounding mandible, tongue, thyroid, and pharynx with suprahyoid and infrahyoid muscles Graber (1978), James and Hiatt (2010). The vertical growth of the hyoid bone is parallel to the vertebra. During growth, it maintains a relatively stable die position between C3 and C4 and moves with the mandible and vertebra Tourné (1991). In the early part of the intrauterine period, the hyoid bone is composed of hyaline cartilage. During its development, it is directly related to the cartilages in the styloid process Pettit and Auvenshine (2018). Its development is completed by the ossification of 6 different centers. Two of them appear in the middle of the cartilage, on the sides of the midline before or immediately after birth and combine to form the bone corpus Parsons (1909). The aim of this study is to evaluate pharyngeal airway measurements and hyoid measurements according to pre-peak, peak and post-peak growth-development periods.
2. MATERIALS AND METHODS
This retrospective clinical study was conducted in the radiographic records of patients who applied to Süleyman Demirel University for treatment between 2018 and 2020. Ethics committee approval was obtained for our study. The study was carried out in accordance with the Principles of the Declaration of Helsinki. An 'Informed Consent Form' and a form stating that the materials can be used in scientific studies and publications are taken from each patient who applies to our clinic for treatment.
The sample size required for the study was calculated with the G*Power analysis (G*Power Ver.3.0.10, Kiel, Germany) at a significance level of 0.05 and a power of 80%, and it was determined that a minimum of 21 individuals were required for each group. More individuals were included in our study in order to increase the power of the study and considering the possible losses.
Selection criteria of radiographs; Schendel et al. (2012) skeletal Class I malocclusion (0<ANB<4), Tourné (1991) no any pathology in the airway, Martin et al. (2011) no any congenital and/or acquired anomaly (cleft lip and palate etc.), Aloufi et al. (2012) detection of reference points properly in initial radiographs and having sufficient image quality, Taylor et al. (1996) the correct position of the head during the lateral cephalometric film is taken.
A total of 531 individuals, 289 female and 242 males, who met the criteria for inclusion according to the above-mentioned criteria were included Table 1. The classification of patients according to pubertal growth spurt periods in grouping according to growth-development period was determined by Lamparski's method from lateral cephalometric films taken at the beginning of treatment Lamparski (1972). Individuals in the CS1 and CS2 periods were divided into the pre-peak group, the individuals in the CS3 and CS4 periods were divided into the peak group, and the individuals in the CS5 and CS6 periods were divided into the post-peak group. Pharyngeal airway measurements and hyoid measurements were compared according to these three different growth-development periods
Lateral cephalometric films included in the study were calibrated on the Planmeca Romexis (Planmeca Romexis Viewer®, Helsinki, Finland) software program and were printed on tracing paper in 1:1 dimension in real size. Then, measurements were made by drawing the following cephalometric points and planes with the help of a 0.3 mm lead pencil. The cephalometric landmarks used in the study are shown in Figure 1, pharyngeal airway measurements in Figure 2, and hyoid measurements in Figure 3.
Figure 1
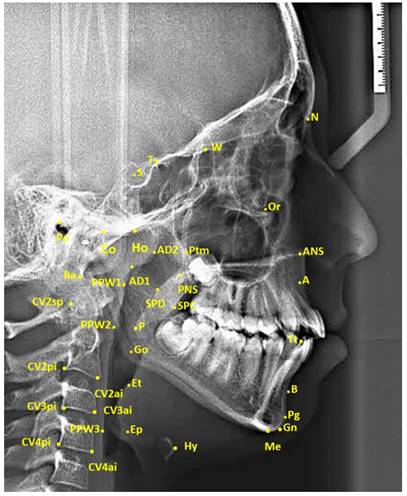
|
Figure 1 The Cephalometric Landmarks |
Area measurements were performed on digital lateral cephalometric films after digital calibration was performed in SketchAndCalc™ software program (SketchAndCalc Area Calculator software, Axiom Welldone ©, https://www.sketchandcalc.com/ . Area measurements are shown in Figure 3.
Figure 2
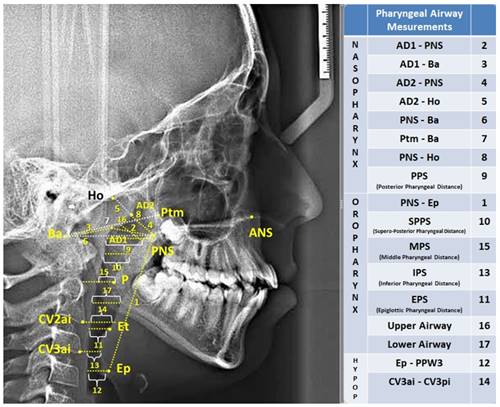
|
Figure 2 Pharyngeal Airway Measurements |
Figure 3
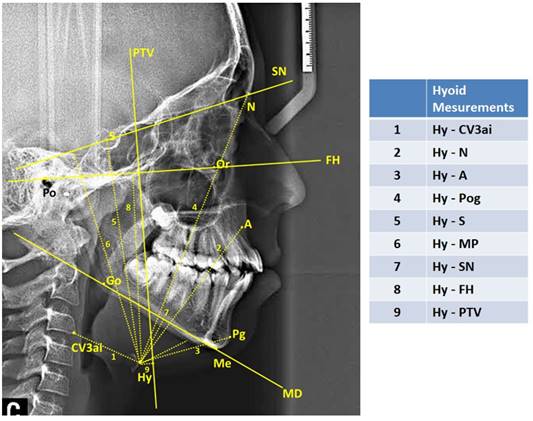
|
Figure 3 Hyoid Measurements |
3. STATISTICAL ANALYSIS
Whether the data had a normal distribution or not was determined by the Kolmogorov-Smirnov test. Parametric tests were used since it was determined that the parameters evaluated in the study were normally distributed. Descriptive statistics are shown as (Mean) ± SD (Standard Deviation). The distribution of gender and growth-development stages of the patients was compared with the Pearson chi-square independence test. One-way ANOVA test was used to evaluate the chronological ages and the mean differences of pharyngeal airway and hyoid measurements made on cephalometric films, and Tukey post-hoc test was used for pairwise comparisons.
In order to determine the method error of the measurements, 145 films were randomly selected from 531 lateral cephalometric films, and the measurements were repeated two weeks later by the same researcher, after blinding. Cronbach α coefficients were determined for each measurement. It was determined that the repeatability coefficients in our measurements were high (α>0.904). SPSS package program (SPSS for Win, veer 21.0; SPSS Inc, Chicago, Ill) was used for data analysis. The results were considered statistically significant at the p<0.05 significance level.
4. RESULTS AND DISCUSSIONS
Table 1 shows the distribution of patients grouped according to growth and development periods, according to chronological age, gender, and cervical vertebra maturation period. When the distribution of individuals in the groups according to the cervical vertebra maturation period was examined; a statistically significant correlation was observed between growth-development periods, and chronological age (p<0.05).
Table 1
|
Table 1 Demographic statistics according to growth and development periods |
||||||
|
Pre-Peak |
Peak |
Post-Peak |
TOTAL |
|||
|
(n=137) |
(n=223) |
(n=171) |
(n=531) |
p |
||
|
Age
+(x̄ ± SD) |
10.43
± 1.57 |
12.17
± 1.09 |
14.86
± 1.85 |
11.73
± 1.75 |
0 |
|
|
Gender * n (%) |
Male |
86
(62.77) |
109 (48.87) |
47
(27.48) |
242
(100) |
NS |
|
Female |
51
(37.23) |
114
(51.13) |
124
(72.52) |
289
(100) |
||
|
Growth-development
period *(n) |
CS
Distribution |
56
CS 1 |
126
CS 3 |
75
CS 5 |
531
(100) |
0 |
|
One-Way Analysis of Variance (ANOVA); *:
Pearson chi-square test |
||||||
When the effects of growth and development periods on the pharyngeal airway are examined, the differences between the pre-peak group and the peak group in the nasopharynx are AD1-PNS (mm), AD2-PNS (mm), PNS-Ba(mm), Ptm-Ba(mm), PNS-Ho (mm), posterior pharyngeal length (PPS) and upper airway measurements defined by McNamara were statistically significant (p<0.05). A statistically significant difference was found between the pre-peak group and the post-peak group in all measurements in the nasopharynx (p<0.05). A statistically significant difference was found between the pre-peak group and the post-peak group in AD1-PNS (mm), AD2-PNS (mm), AD1-Ba(mm), AD2-Ho(mm) and posterior pharyngeal length (p<0.05) Table 2.
In the oropharynx part of the airway measurements, a statistically significant difference was found only in the vertical airway length PNS-Ep(mm) between the pre-peak group and the peak group (p<0.05). A statistically significant difference was found between the pre-peak group and the post-peak group in PNS-Ep(mm), upper posterior airway length (SPPS), epiglottic airway length (EPS), and lower pharyngeal length (IPS) (p<0.05). A statistically significant difference was found between the pre-peak group and the post-peak group in PNS-Ep(mm) and lower pharyngeal length (IPS) (p<0.05) Table 2.
Table 2
|
Table 2 Comparison of airway measurements by growth development period |
||||||||
|
|
|
Group
1 Pre-Peak |
Group
2 Peak |
Group
3 Post-Peak |
Tukey
Test |
ANOVA |
||
|
|
|
(x̄
± SD) |
(x̄
± SD) |
(x̄
± SD) |
2-Jan |
3-Jan |
3-Feb |
p |
|
Airway
Measurements |
PNS-Ep |
50.29±5.43 |
55.77±6.78 |
60.13±6.75 |
0 |
0 |
0 |
0 |
|
AD1-PNS |
20.23±4.62 |
22.71±5.01 |
24.09±5.04 |
0 |
0 |
0.017 |
0 |
|
|
AD1-Ba |
21.13±4.47 |
21.32±4.48 |
19.33±4.02 |
NS |
0.001 |
0 |
0 |
|
|
AD2-PNS |
15.69±3.45 |
17.56
± 3.87 |
19.97±4.53 |
0 |
0 |
0 |
0 |
|
|
AD2-Ho |
12.40±4.15 |
11.95±3.81 |
9.88±4.11 |
NS |
0 |
0 |
0 |
|
|
PNS-Ba |
41.39±5.06 |
43.72±5.09 |
43.37±5.33 |
0 |
0.003 |
NS |
0 |
|
|
Ptm-Ba |
36.93±4.78 |
39.20±4.18 |
39.27±3.55 |
0 |
0 |
NS |
0 |
|
|
PNS-Ho |
27.96±3.85 |
29.83±4.26 |
30.12±3.84 |
0 |
0 |
NS |
0 |
|
|
PPS |
21.12±4.73 |
24.06±5.27 |
25.40±5.18 |
0 |
0 |
0.027 |
0 |
|
|
SPPS |
9.32±3.00 |
9.66±2.76 |
10.32±2.84 |
NS |
0.007 |
NS |
0.007 |
|
|
EPS |
10.15±2.98 |
10.73±3.13 |
11.06±3.31 |
NS |
0.034 |
NS |
0 |
|
|
IPS |
11.37±4.05 |
12.06±4.23 |
13.92±4.15 |
NS |
0 |
0 |
0.713 |
|
|
MPS |
12.19±3.25 |
12.36±3.60 |
12.06±3.83 |
NS |
NS |
NS |
0 |
|
|
Upper
Airway |
6.38±2.26 |
7.15±2.43 |
7.72±2.61 |
0.01 |
0 |
NS |
0 |
|
|
Lower
Airway |
10.02±3.04 |
10.19±2.85 |
10.03±3.35 |
NS |
NS |
NS |
0.826 |
|
|
Hyoid
Measurements |
Hy-CV3ai |
29.48±4.11 |
31.13±4.69 |
32.23±4.82 |
0.003 |
0 |
0.05 |
0 |
|
Hy-
A |
64.31±5.91 |
69.22±8.17 |
73.26±7.17 |
0 |
0 |
0 |
0 |
|
|
Hy-Pog |
41.86±5.86 |
44.58±6.19 |
47.73±6.14 |
0 |
0 |
0 |
0 |
|
|
Hy-
N |
106.69±7.42 |
114.01±9.05 |
119.35±9.37 |
0 |
0 |
0 |
0 |
|
|
Hy-S |
87.75±8.17 |
94.32±9.50 |
97.81±11.76 |
0 |
0 |
0.002 |
0 |
|
|
Hy-SN |
88.44±7.53 |
94.81±8.25 |
99.35±9.64 |
0 |
0 |
0 |
0 |
|
|
Hy-MP |
10.07±4.38 |
12.35±5.19 |
13.72±5.19 |
0 |
0 |
0.019 |
0 |
|
|
Hy-
FH |
69.37±6.92 |
75.27±7.78 |
79.98±8.08 |
0 |
0 |
0 |
0 |
|
|
Hy-PTV |
0.84±6.55 |
-0.32±6.81 |
-0.19±7.06 |
NS |
NS |
NS |
0.258 |
|
|
Area
Measurements |
Oropharynx
Area |
397.95±131.15 |
444.74±114.21 |
506.51±145.72 |
0.003 |
0 |
0 |
0 |
|
Nasopharynx
Area |
89.94±47.26 |
110.99±56.09 |
138.24±64.11 |
0.002 |
0 |
0 |
0 |
|
|
Hypopharynx
Area |
176.82±80.85 |
202.67±81.89 |
233.39±88.28 |
0.013 |
0 |
0.001 |
0 |
|
|
Total
Area |
664.72±193.74 |
758.41±180.40 |
878.14±213.33 |
0 |
0 |
0 |
0 |
|
|
|
x̄: Mean; SD: Standard Deviation; P: One-Way Analysis of Variance (ANOVA); NS: not-significant
p>0.05 |
|||||||
A statistically significant difference was found in all three groups divided according to growth and development periods in all of the hyoid measurements, except for the Hy - PTV (mm) measurement, which we evaluated the position of the hyoid bone, where we evaluated the position of the hyoid bone in the sagittal plane (p<0.05).
Finally, when the area measurements were examined, a statistically significant difference was found in all area measurements (oropharynx area, nasopharyngeal area, hypopharyngeal area) of the structures forming the airway in three groups divided according to growth and development periods (p<0.05) Table 2.
Skeletal development is evaluated rather than chronological age to determine the growth-development period Proffit et al. (2007). For this purpose, CVM period is frequently used on hand-wrist films and mostly lateral cephalometric films. The method we preferred in our study was to determine the skeletal maturation period from the lateral cephalometric films taken at the beginning of the treatment and which we will use for our measurements. With this method, patients are not exposed to additional radiation for growth-development detection. CVM period is preferred in cases where it is necessary to determine the growth and development in order not to exceed the total radiation dose, since it is found to be high in reproducibility in studies. In order to determine the CVM period, the Lamparski method Lamparski (1972) was used to divide the individuals in the CS1 and CS2 periods into the pre-peak group, the individuals in the CS3 and CS4 periods into the peak group, and the individuals in the CS5 and CS6 periods in the post-peak group. According to these three different growth-development stages, pharyngeal airway measurements and hyoid measurements were compared.
When the literature was examined, no study was found that evaluated the pharyngeal airway dimensions and the position of the hyoid bone according to different growth and development periods. Tsai et al in 2007, examined the development according to the dentition period Tsai et al. (2007). Airway dimensions of individuals divided into 3 groups as early mixed dentition, early permanent dentition and permanent dentition were examined. In 2016, Akçam divided individuals with Class II malocclusion into different developmental periods according to hand-wrist films and examined airway dimensions. Apart from these studies, there is no study with which we can compare our findings. That's why; since the growth-development periods show parallelism with age, it was associated with age when examining our findings.
In two-dimensional studies to examine the changes in pharyngeal dimensions with growth; Bench, Tourne, and King reported that in the early stages of life, the nasopharynx grows mostly in the vertical direction, and the increase in the anteroposterior direction is quite low. They stated that the changes in the airway in the period after pubertal excretion were minimal Tourné (1991), Bench (1963), King (1952)
Arat and Erdem investigated whether the position of the mandibule and the height of the face are affected by the nasopharyngeal and oropharyngeal airway dimensions in their study on lateral cephalometric films of 40 individuals in the prepubertal and postpubertal period and nasal breathing. According to the research, no significant correlation was found between nasopharynx and oropharynx area and other measurements in prepubertal girls, postpubertal boys and girls. However, they suggested that there is a negative significant relationship between the angle between the palatal plane and the mandibular plane with the naso-oropharynx in prepubertal men Erdem and Arat (1991)
Hypertrophy of the adenoid tissue causes narrowing of the nasopharyngeal airway. Adenoid tissues grow until 14-15 years of age, and then gradually shrink to reaching adult size Odar (1978), Handelman and Osborne (1976) Similarly, the palatine tonsils in the oropharynx reach their maximum size during puberty and shrink after puberty Çoban (2014). After the 11-14 age group of the individuals included in our study, reduction in adenoid tissues (AD1-Ba, AD2-Ho), nasopharynx (AD1-PNS, AD2-PNS, PPS) and oropharyngeal dimensions (PNS-Ep, SPPS, EPS, Upper Airway) an increase was observed.
While it is emphasized in the literature that the pharyngeal structures continue to grow rapidly until the age of 13 Jeans et al. (1981), it has been reported that there is a stable period for the pharyngeal structures between the ages of 14 and 18 Taylor et al. (1996). In a longitudinal study conducted between the ages of 22 and 42, it was stated that the pharyngeal region narrows with age, while the soft palate becomes longer and thicker Kollias and Krogstad (1999).
Bench examined the position of the hyoid bone longitudinally from the age of three to adulthood and suggested that the Hy-MD measurement was 12 mm at the age of 12, with an annual increase of 0.78 mm Bench (1963).
Mitani et al. compared the growth characteristics of the hyoid bone, height, wrist bones and cervical vertebrae with the growth characteristics of the mandible during puberty Mitani and Sato (1992). The study was conducted on 33 girls between the ages of 9 and 14. According to the findings, the hyoid bone did not correlate with other parameters at any age. They also reported that there were different development rates between the mandible and the hyoid bone compared to other parameters. They argued that there are strong correlations between height and wrist bones and cervical vertebrae, as well as between bone length and length of hand bones. However, they stated that there was no significant relationship between mandibular growth and hyoid bone growth, and that the growth rate increased at most in all parameters at the age of 9, 10, and 11 years.
Akçam and Uslu divided 45 individuals with Class II malocclusion into different developmental stages according to hand-wrist films and examined airway dimensions Akçam (2017). As a result of the study, there was a statistically significant increase in nasopharyngeal airway dimensions from prepubertal period to adulthood, but no significant change was observed in oropharyngeal airway dimensions. In our study, a significant increase was observed in both nasopharyngeal and oropharyngeal airway dimensions as the growth-development period progressed.
Tsai et al., on the other hand, examined the development according to the dentition period. Airway dimensions of individuals divided into 3 groups as early mixed dentition, early permanent dentition and permanent dentition were examined. As a result, they found that the upper airway dimensions increased with age, but the lower airway dimensions were greater in the early period. They found that the pharyngeal airway capacity increased with vertical growth and the increase in men was higher than in women Tsai et al. (2007). In our study, while a significant increase was observed in most of the airway parameters until the peak period, an increase in some parameters from the peak period to the post-peak period was detected in some parameters. In addition, as the growth and development period of the individuals progressed, an increase in the pharyngeal airway area, and a downward and backward movement in the hyoid position were observed.
5. CONCLUSIONS AND RECOMMENDATIONS
With age and as the growth-development periods progress, the dimensions of the pharyngeal airway increase, and the hyoid bone moves downwards.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
None.
REFERENCES
Akçam, Ö.U. (2017). İskeletsel sınıf II bireylerde nazofarengeal havayolunun farklı gelişim dönemlerinde değerlendirilmesi. Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi, 27(1), 1-6. https://doi.org/10.17567/ataunidfd.307084
Aloufi, F. Preston, C.B. Zawawi, K.H. (2012). Changes in the upper and lower pharyngeal airway spaces associated with rapid maxillary expansion. https://doi.org/10.5402/2012/290964
Bench, R.W. (1963). Growth of the cervical vertebrae as related to tongue, face, and denture behavior. American Journal of Orthodontics, 49(3), 183-214. https://doi.org/10.1016/0002-9416(63)90050-2
Çoban, D.E. (2014). Farklı malokluzyona sahip bireylerde farengeal havayolu hacminin üç boyutlu olarak incelenmesi. Dicle Üniversitesi Sağlık Bilimleri Enstitüsü, Doktora Tezi, Diyarbakır. http://acikerisim.dicle.edu.tr/xmlui/handle/11468/812
Demiray, D. Günay, N. (1987). Naso-orofarenks alanı ile üst çene boyutları arasındaki ilişkilerin incelenmesi. Ankara Üniversitesi Sağlık Bilimleri Enstitüsü, Doktora Tezi, Ankara. https://dspace.ankara.edu.tr/xmlui/handle/20.500.12575/34744
Erdem, D. Arat, M. (1991). Naso-Orofarenks, mandibula konumu ve yüz yüksekligi. A Ü Dis, Hek Fak Derg, 99-108.
Graber, L.W. (1978). Hyoid changes following orthopedic treatment of mandibular prognathism, 48(1), 33-38. https://europepmc.org/article/med/272129
Handelman, C.S. Osborne, G. (1976). Growth of the nasopharynx and adenoid development from one to eighteen years. The Angle Orthodontist, 46(3), 243-59.
James, L. Hiatt, L.P.G. (2010). The Oral Cavity, Palate,and Pharynx. Textbook of Head and Neck Anatomy, 49.
Jeans, W. Fernando, D. Maw, A. Leighton, B. (1981). A longitudinal study of the growth of the nasopharynx and its contents in normal children. The British Journal of Radiology, 54(638), 117-21. https://doi.org/10.1259/0007-1285-54-638-117
King, E.W. (1952). A roentgenographic study of pharyngeal growth. The Angle Orthodontist,22(1), 23-37.
Kollias, I. Krogstad, O. (1999). Adult craniocervical and pharyngeal changes-a longitudinal cephalometric study between 22 and 42 years of age. Part 1: morphological craniocervical and hyoid bone changes. The European Journal of Orthodontics, 21(4), 333-44. https://doi.org/10.1093/ejo/21.4.333
Lamparski, D. (1972). Skeletal age assessment utilizing cervical vertebrae. University of Pittsburgh, School of Dental Medicine, Master of dental science thesis, Pittsburgh. https://cir.nii.ac.jp/crid/1570291224971419264
Martin, O. Muelas, L. Vinas, M.J. (2011). Comparative study of nasopharyngeal soft-tissue characteristics in patients with Class III malocclusion. Am J Orthod Dentofacial Orthop, 242-51. https://doi.org/10.1016/j.ajodo.2009.07.016
Mitani, H. Sato, K. (1992). Comparison of mandibular growth with other variables during puberty. The Angle Orthodontist, 62(3), 217-22. https://pubmed.ncbi.nlm.nih.gov/1416242/
Odar, İ.V. (1978).
Anatomi Ders Kitabı. 2th Ed., Ankara : Elif matbaacılık, 58- 68.
Parsons, F. (1909). The topography and morphology of the human hyoid bone. Journal of Anatomy Physiology, 279. https://pubmed.ncbi.nlm.nih.gov/17232809/
Pettit, N.J. Auvenshine, R.C. (2018). Change of hyoid bone position in patients treated for and resolved of myofascial pain, 1-17. https://doi.org/10.1080/08869634.2018.1493178
Proffit, W.R. Fields, H.W. Sarver, D.M. (2007). Contemporary Orthodontics. 5th Ed., St. Louis, Missouri : Mosby Elsevier, 81-86.
Schendel, S.A. Jacobson, R. Khalessi, S. (2012). Airway growth and development: a computerized 3-dimensional analysis, 70(9),2174-83. https://doi.org/10.1016/j.joms.2011.10.013
Taylor, M. Hans, M.G. Strohl, K.P. Nelson, Broadbent, S.H. (1996). Soft tissue growth of the oropharynx. Angle Orthod, 66(5),393-400.
Tourné, L.P. (1991). Growth of the pharynx and its physiologic implications, 99(2), 129-39. https://doi.org/10.1016/0889-5406(91)70115-D
Tsai, H-H. Ho, C-Y. Lee, P-L. Tan, C-T. (2007). Cephalometric analysis of nonobese snorers either with or without obstructive sleep apnea syndrome. The Angle Orthodontist,77(6), 1054-61. https://doi.org/10.2319/112106-477.1
Vig, P. (1974). The size of the tongue and the intermaxillary space. Angle Orthod, 44, 25-8.
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2022. All Rights Reserved.

