
ASSESSING WAIST-HIP RATIO AND BODY MASS INDEX AS RISK FACTORS FOR CARDIOVASCULAR EVENTS IN INDIVIDUALS WITH CHRONIC KIDNEY DISEASE
Nithinchandra Kini N 1, Dr. Madhava Reddy Kurapati 2
1 Research
Scholar, Department of Physiotherapy, SunRise
University, Alwar, Rajasthan, India
2 Professor,
Department of Physiotherapy, SunRise University,
Alwar, Rajasthan, India
|
|
|
ABSTRACT |
|
|
The purpose of
the research was to assess how well physiotherapy interventions, such as the
Romson's Respirometer and Pursed Lip Breathing (PLB) exercises, can enhance
the quality of life for emphysema patients. The goal was to evaluate the
efficacy of various therapies, the prevalence of emphysema, and demographic
factors. Using a comparative study of treatment results based on
quality-of-life variables, a sample of one hundred patients was used. The
quality of life for individuals using both therapies significantly improved,
according to the data, with Romson's Respirometer demonstrating marginally
better outcomes than PLB exercises. The conclusion highlights the usefulness
of both physiotherapy interventions in the management of emphysema and
recommends their inclusion in routine care regimens to improve patient
outcomes and quality of life. |
|||
|
Received 30 October
2024 Accepted 15 November 2024 Published 30 November 2024 DOI 10.29121/granthaalayah.v12.i11.2024.6762 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2024 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Pursed Lip Breathing, Romson's
Respirometer, Physiotherapy, Emphysema, Therapies, Chronic Kidney Disease,
Cardiovascular |
|||
1. INTRODUCTION
In the US, the frequency and pervasiveness of chronic kidney disease (CKD) are rising, influencing around 13% of the population. coronary illness CKD is currently perceived to be a different gamble factor for MI and cardiovascular death. The quantity of individuals with CKD is ascending because of the maturing populace's increasing paces of diabetes and hypertension. Cardiovascular disease is the primary driver of mortality for those with CKD, similarly for all intents and purposes for everyone. Furthermore, in everyone, heftiness raises the gamble of death from CVD. Throughout the course of recent many years, there has been a critical expansion in the quantity of grown-up Americans who experience the ill effects of corpulence. As per the latest measurements that anyone could hope to find from the Public Community for Wellbeing Measurements, 30% of American grown-ups — or north of 60 million individuals — are fat. It is muddled, thusly, what stoutness means for people with CKD as far as hazard factors for MI and passing. Clashing discoveries from prior research utilizing weight list BMI to survey heftiness as a gamble factor for troublesome results in CKD have been reported, which might be because of the impact of bone, fat, and bulk on BMI. Diminished instinctive fat (and decreased CVD risk) or diminished bulk (and more prominent CVD risk) may both be reflected in lower BMI in CKD, where muscle squandering is boundless. The net effect of BMI on results relies upon the corresponding commitments of both. Contrasted with other anthropometric measures, like BMI, midriff to hip proportion WHR, which estimates instinctive fat and focal heftiness, might be a more exact sign of stoutness since high WHR can show both an overall absence of gluteal muscle and an expansion in instinctive fat, the two of which have been viewed as freely connected with cardiovascular disease risk. WHR might be a more precise mark of weight risk in a gathering with a high occurrence of muscle deficit and unhealthiness, like those with CKD, since it is a more delicate measure for focal corpulence and might be less influenced by bulk. To look at WHR and BMI as chance elements for MI and cardiovascular passing in individuals with CKD, we did as such.
2. LITERATURE REVIEW
Hsuan et al. (2022) found a more accurate anthropometric measure to predict cardiovascular events in ASCVD patients. The Taiwanese Optional Prevention for patients with AtheRosCLErotic sickness (T-SPARCLE) Library was utilized in the exploration. 73.9% of the 6,920 grown-up patients with stable ASCVD who were incorporated between January 2010 and November 2014 had a mean time of 65.9 years, a mean BMI of 26.3 kg/m2, and a mean period of 65.9 years at gauge. The patients went through a middle subsequent time of 2.5 years. The composite major adverse cardiovascular event (MACE), which incorporates heart failure with revival, nonfatal myocardial localized necrosis or stroke, and cardiovascular mortality, was the review's endpoint. In the wake of controlling for putative gamble factors and confounders, multivariable Cox corresponding dangers relapse uncovered a huge positive connection between's waist-to-BMI ratio and MACE (changed risk ratio 1.69 per cm‧m2/kg expansion in waist-to-BMI ratio, 95% CI 1.12-2.49, p = 0.01). There were no genuinely huge direct connections found between more established waist-based files like body roundness record and body structure file and later waist-based lists like BMI, weight, waist, and waist-hip ratio.
Betzler et al. (2021) studies, adult men, non-smokers, and those with diabetes and arterial hypertension showed significant relationships between BMI and CKD (all p<0.05). In a continuous variable analysis, there was no significant correlation found between BMI and CKD. Given that CKD and obesity are two of the world's most common chronic illnesses with significant public health burdens, if these findings hold up in long-term research, they may have therapeutic ramifications for risk assessment and preventative interventions.
Hung et al. (2022) connected to the development of renal function. The obesity paradox for renal outcomes, however, refers to some research linking a high body mass index (BMI) to better renal outcomes, particularly in advanced chronic kidney disease (CKD). The obesity paradox in all-cause mortality may be explained by central obesity. It is unclear, nevertheless, whether obesity or central obesity is linked to renal outcomes in individuals with severe chronic kidney disease (CKD), such as renal replacement therapy or a 50% drop in estimated glomerular filtration rate. 3605 Asian patients with CKD stages 1–5 were enrolled in our research; they were split into six groups based on their BMI, which ranged from 15 to 35 kg/m2. At CKD stages 4 and 5, BMI was positively correlated with both hemoglobin and albumin using linear regression. A high BMI was linked to renal outcomes at CKD stages 1-3 in the competing risk Cox regression model, but not at stages 4 or 5. Renal outcomes were linked to a high BMI in individuals with hemoglobin levels ≥11 g/dL, but not less than that. There was no correlation between renal outcomes and a high waist-to-hip ratio. We conclude that the obesity paradox in renal outcomes in individuals with CKD may be explained by the anemia and stage of the disease.
Memarian et al. (2021) This huge scope imminent review set off on a mission to explore, in a populace-based companion study, the relationship between different anthropometric proportions of heftiness, for example, body mass index (BMI), waist circumference (WC), waist circumference to level ratio (WHtR), waist-to-hip ratio (WHR), level of body fat (BF%), weight, level, and occurrence of hospitalizations because of chronic kidney disease (CKD). From 1991 to 1996, the Swedish "Malmö Diet and Malignant growth Study (MDCS)" associate was examined. A total of 28,449 members finished a poll, had their pulse and anthropometric estimations taken, and both. Over a mean development of 18 years, the recurrence of long term and short-term emergency clinic visits for CKD was followed from the benchmark evaluation.
Song et al. (2022) surveyed the gamble of creating chronic kidney disease (CKD) in a moderately aged partner comparable to a few body synthesis measures. We included 6727 moderately aged individuals who had benchmark and follow-up information accessible from an imminent partner of 10,030. The people were ordered into quintiles in light of the data we accumulated about their BMI, actually evaluated waist-hip ratio (WHR), and other bioelectrical impedance analysis (BIA) boundaries, for example, total body fat substance, muscle content, and assessed WHR. In ensuing laboratory testing, chronic kidney disease (CKD) was named an expected glomerular filtration rate. Total body muscle expanded the gamble of CKD, yet increments in BMI, WHR, and total body fat were connected to an upgraded risk. Not set in stone by BIA displayed the best prescient incentive for CKD (C-insights: 0.615) of all the body organization estimations. Besides, contrasted with those with "typical weight corpulence," which is described as high WHR however a typical BMI, the people who were "sound overweight," or had a low WHR yet a high BMI, had a 62% diminished possibility of getting CKD.
3. METHODOLOGY
3.1. Research Design
In order to evaluate the association between Waist-Hip Ratio (WHR) and Body Mass Index (BMI) as risk factors for cardiovascular events in people with Chronic Kidney Disease (CKD), this study used a quantitative research approach. One method for gathering numerical data from a particular population at one moment in time is the cross-sectional technique. Body composition measures (WHR and BMI) and the incidence of cardiovascular problems may be correlated, thanks to this design's ability to quantify variables and perform statistical analysis. The research intends to provide objective and quantifiable insights into how these risk variables affect cardiovascular health in people with chronic kidney disease (CKD) by using quantitative approaches.
3.2. Data Collection Techniques
Systematic approaches are used in data collecting to guarantee precise measurement and evaluation. WHR and BMI of individuals are assessed by anthropometric measures. While BMI is computed using the formula BMI = weight (kg) / height (m2), WHR is measured using a flexible measuring tape. A comprehensive assessment of medical data is carried out to discover any previous incidences, such as heart attacks or strokes, in order to evaluate cardiovascular events. Standardized questionnaires are also used to gather other health-related data, such as medical history and demographics. The legitimacy and unwavering quality of the information accumulated are worked on by the utilization of organized polls related to true measures.
3.3. Sample Size
A total of 100 people with chronic kidney disease were included in the study's sample. To provide a varied representation of the CKD community, participants were chosen from nephrology wards and outpatient clinics located across many institutions. The sample size of this study was judged enough for statistical analysis, allowing for the investigation of potential correlations between WHR, BMI, and cardiovascular events. Additionally, this increased the generalizability of the results to a larger population with chronic kidney disease.
3.4. Data Analysis
Quantitative approaches were used in data analysis to get significant insights from the gathered data. In order to compile the frequencies and percentages for the WHR and BMI categories as well as the participant demographics, descriptive statistics were generated. We used inferential statistical techniques, namely chi-square tests, to evaluate the associations between cardiovascular event incidence and WHR and BMI categories. A p-worth of under 0.05 was utilized as the limit for factual importance. To distinguish conceivable gamble factors and further our insight into cardiovascular wellbeing in individuals with chronic kidney disease (CKD), our quantitative examination looked to recognize patterns in the frequencies of cardiovascular events across different WHR and BMI gatherings.
4. DATA ANALYSIS
Among the 100 people with chronic kidney disease (CKD), the distribution of Waist-Hip Ratio (WHR) categories provides significant information about prospective cardiovascular risk factors.
Table 1
|
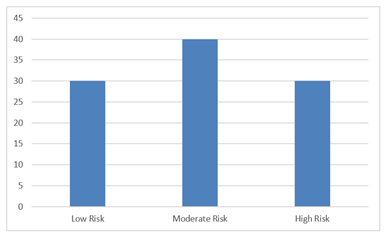
Table 1 Distribution of Waist-Hip Ratio (WHR) Categories |
||
|
WHR Category |
Total (n=100) |
Percentage (%) |
|
Low Risk |
30 |
30 |
|
Moderate Risk |
40 |
40 |
|
High Risk |
30 |
30 |
Figure 1
|
Figure 1 Graphical Representation on the Percentage of Distribution of Waist-Hip Ratio (WHR) Categories |
According to the statistics, 30% of participants are classified as low-risk, meaning that a sizeable segment of the population maintains a better WHR, which is linked to a decreased risk of cardiovascular disease. However, 40% of the individuals fall into the moderate-risk group, indicating that a sizeable portion of the population is more vulnerable to cardiovascular events as a result of having an intermediate WHR. At last, 30% of members are delegated high gamble, implying that 33% of the members had a WHR connected to an expanded gamble of cardiovascular issues. In rundown, the information demonstrates that a critical extent of people with chronic kidney disease (CKD) are at moderate to high gamble of cardiovascular events. This highlights the need of centered medicines that endeavor to oversee waist-hip ratios to lessen the probability of cardiovascular issues in this vulnerable gathering.
Table 2
|
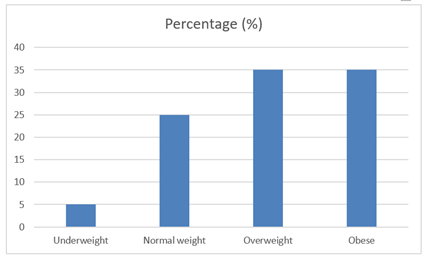
Table 2 Distribution of Body Mass Index (BMI) Categories |
||
|
BMI Category |
Percentage (%) |
|
|
Underweight |
5 |
5 |
|
Normal weight |
25 |
25 |
|
Overweight |
35 |
35 |
|
Obese |
35 |
35 |
Figure 2
|
Figure 2 Graphical Representation on the Percentage of Body Mass Index (BMI) Categories |
There are notable differences in the weight status of the 100 people with chronic kidney disease (CKD) based on the distribution of Body Mass Index (BMI) categories. Merely 5% of the subjects are categorized as underweight, suggesting that a very small proportion of people are underweight. On the other hand, 25% of the participants are classified as normal weight, indicating that a moderate segment of the population keeps their BMI within a healthy range. Nonetheless, a significant 35% are categorized as overweight, and an equivalent 35% as obese. Concerns are raised by the high incidence of overweight and obesity among CKD patients since these BMI categories are linked to higher risks for a number of health issues, including cardiovascular disease. To address the high paces of overweight and stoutness locally, custom-made weight the executives and mediation measures are required. Doing so might greatly improve the population's overall health outcomes and lower the chance of developing new problems.
Table 3
|
Table 3 Cardiovascular Events by WHR and BMI Categories |
||||
|
WHR Category |
Cardiovascular Events (Yes) |
Cardiovascular Events (No) |
Total (n=100) |
Percentage of Events (%) |
|
Low Risk |
5 |
25 |
30 |
16.7 |
|
Moderate Risk |
15 |
25 |
40 |
37.5 |
|
High Risk |
20 |
10 |
30 |
66.7 |
Table 3 presents information that demonstrates serious areas of strength for a between the frequency of cardiovascular events and the Waist-Hip Ratio (WHR) classifications among the 100 patients with chronic kidney disease (CKD). Just 5 out of 30 individuals who were categorized as low risk had cardiovascular events, yielding a comparatively low occurrence rate of 16.7%. On the other hand, a substantial rise in cardiovascular events was seen in the moderate-risk group (15 out of 40 individuals), which resulted in a much higher proportion of 37.5%. Above all, the high-risk group showed the highest correlation—20 out of 30 participants had cardiovascular events, or an astounding 66.7% of all occurrences. Overall, the findings highlight the vital role of WHR as a risk factor in this group by showing that the prevalence of cardiovascular events rises with the WHR risk category. This result emphasizes the need for attentive monitoring and methods for intervention that target waist-hip ratios in order to reduce cardiovascular risks in individuals with chronic kidney disease.
Table 4
|
Table 4 Cardiovascular Events by BMI Categories |
||||
|
BMI Category |
Cardiovascular Events (Yes) |
Cardiovascular Events (No) |
Total (n=100) |
Percentage of Events (%) |
|
Underweight |
0 |
5 |
5 |
0 |
|
Normal weight |
5 |
20 |
25 |
20 |
|
Overweight |
15 |
20 |
35 |
42.9 |
|
Obese |
20 |
15 |
35 |
57.1 |
Table 4 presents the connection between the occurrence of cardiovascular events among 100 persons with chronic kidney disease (CKD) and the categories of Body Mass Index (BMI). Interestingly, among the five individuals who were categorized as underweight, there were no cardiovascular events recorded; hence, the event rate for this group was 0%. Twenty percent of the patients in the normal weight group (20 out of 25) had cardiovascular incidents. In the overweight group, where 15 out of 35 patients (42.9%) had cardiovascular problems, the pattern of rising risk is more evident. In the obese group, where 20 out of 35 people (57.1%) suffered cardiovascular problems, this tendency is still greatly increasing. Overall, the findings point to a strong relationship between CKD patients' greater BMI and higher risk of cardiovascular events, with obesity carrying the greatest risk. These results underline the critical need for efficient weight-management plans and programs that minimize obesity and lower cardiovascular risk in this susceptible group.
5. CONCLUSION
The current examination features the significant connection between's the WHR and the frequency of cardiovascular events in patients determined to have CKD. The outcomes recommend that there is a positive connection between's a more prominent WHR and a higher gamble of cardiovascular complexities, with a staggering event pace of 66.7% in the high-risk bunch. Moreover, the high pace of stoutness and overweight in the CKD populace underscores the basic requirement for centered treatments intended to control cardiovascular gamble and improve body piece. In light of everything, our discoveries feature the meaning of following WHR notwithstanding ordinary estimates like BMI to all the more precisely decide cardiovascular gamble and set up as a regular occurrence reasonable wellbeing rehearses for CKD patients.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
None.
REFERENCES
Bae, E. H., Lim, S. Y., Jung, J. H., Oh, T. R., Choi, H. S., Kim, C. S., … Kim, S. W. (2021). Obesity, Abdominal Obesity and Chronic Kidney Disease in Young Adults: A Nationwide Population-Based Cohort Study. Journal of Clinical Medicine, 10(5), 1065. https://doi.org/10.3390/jcm10051065
Bae, E. H., Lim, S. Y., Yang, E. M., Oh, T. R., Choi, H. S., Kim, C. S., … Kim, S. W. (2022). Low Waist Circumference Prior to Percutaneous Coronary Intervention Predicts the Risk for End-Stage Renal Disease: A Nationwide Korean Population-Based Cohort Study. The Korean Journal of Internal Medicine, 37(3), 639–650. https://doi.org/10.3904/kjim.2021.313
Betzler, B. K., Sultana, R., Banu, R., Tham, Y. C., Lim, C. C., Wang, Y. X., … Sabanayagam, C. (2021). Association between Body Mass Index and Chronic Kidney Disease in Asian Populations: A Participant-Level Meta-Analysis. Maturitas, 154, 46–54. https://doi.org/10.1016/j.maturitas.2021.09.005
Held, C., Hadziosmanovic, N., Aylward, P. E., Hagström, E., Hochman, J. S., Stewart, R. A., … Wallentin, L. (2022). Body Mass Index and Association with Cardiovascular Outcomes in Patients with Stable Coronary Heart Disease: A STABILITY Substudy. Journal of the American Heart Association, 11(3), e023667. https://doi.org/10.1161/JAHA.121.023667
Hsuan, C. F., Lin, F. J., Lee, T. L., Yang, K. C., Tseng, W. K., Wu, Y. W., … Wu, C. C. (2022). The waist-to-body Mass Index Ratio as an Anthropometric Predictor for Cardiovascular Outcome in Subjects with Established Atherosclerotic Cardiovascular Disease. Scientific Reports, 12(1), 804. https://doi.org/10.1038/s41598-021-04650-5
Hung, C. C., Yu, P. H., Niu, S. W., Kuo, I. C., Lee, J. J., Shen, F. C., … Hwang, S. J. (2022). Association between Body Mass Index and Renal Outcomes Modified by Chronic Kidney Disease and Anemia: The Obesity Paradox for Renal Outcomes. Journal of Clinical Medicine, 11(10), 2787. https://doi.org/10.3390/jcm11102787
Ke, J. F., Wang, J. W., Lu, J. X., Zhang, Z. H., Liu, Y., and Li, L. X. (2022). Waist-to-height Ratio has a Stronger Association with Cardiovascular Risks than Waist Circumference, Waist-Hip Ratio and Body Mass Index in type 2 diabetes. Diabetes Research and Clinical Practice, 183, 109151. https://doi.org/10.1016/j.diabres.2021.109151
Kim, C. S., Han, K. D., Choi, H. S., Bae, E. H., Ma, S. K., and Kim, S. W. (2020). Association of Body Mass Index and Waist Circumference with all-cause Mortality in Hemodialysis Patients. Journal of Clinical Medicine, 9(5), 1289. https://doi.org/10.3390/jcm9051289
Li, Y., He, Y., Yang, L., Liu, Q., Li, C., Wang, Y., … Huang, X. (2022). Body Roundness Index and Waist–Hip Ratio Result in Better Cardiovascular Disease Risk Stratification: Results from a Large Chinese Cross-Sectional Study. Frontiers in Nutrition, 9, 801582. https://doi.org/10.3389/fnut.2022.801582
Memarian, E., Nilsson, P. M., Zia, I., Christensson, A., and Engström, G. (2021). The Risk of Chronic Kidney Disease in Relation to Anthropometric Measures of obesity: A Swedish Cohort Study. BMC Nephrology, 22, 1–10. https://doi.org/10.1186/s12882-021-02531-7
Oliveira, C., Pereira, P. M. D. L., Soares, I. T., Monteiro, M. G., Bastos, M. G., and Cândido, A. P. C. (2020). Cardiovascular Risk Factors in Patients with Chronic Kidney Disease Under Conservative Treatment. International Journal of Cardiovascular Sciences, 34(2), 170–178. https://doi.org/10.36660/ijcs.20190195
Shen, F. C., Chen, M. E., Wu, W. T., Kuo, I. C., Niu, S. W., Lee, J. J., … Hwang, S. J. (2022). Normal Weight and Waist Obesity Indicated by Increased Total Body Fat Associated with all-cause Mortality in stage 3–5 Chronic Kidney Disease. Frontiers in Nutrition, 9, 982519. https://doi.org/10.36660/ijcs.20190195
Shen, F. C., Chiu, Y. W., Kuo, M. C., Lin, M. Y., Lee, J. J., Hwang, S. J., … Chen, H. C. (2021). U-Shaped Association between Waist-to-hip Ratio and all-Cause Mortality in Stage 3–5 Chronic Kidney Disease Patients with Body Mass Index Paradox. Journal of Personalized Medicine, 11(12), 1355. https://doi.org/10.3390/jpm11121355
Song, Y., Hwang, J. A., Shin, J., Cho, E., Ahn, S. Y., Ko, G. J., … Kim, J. E. (2022). Waist–Hip Ratio Measured by Bioelectrical Impedance Analysis as a Valuable Predictor of Chronic Kidney Disease Development. BMC Nephrology, 23(1), 349. https://doi.org/10.1186/s12882-022-02981-7
Yang, Y., Zhang, H., Lan, X., Qin, X., Huang, Y., Wang, J., … Liang, M. (2023). Low BMI and High Waist-To-Hip Ratio are Associated with Mortality Risk Among Hemodialysis Patients: A Multicenter Prospective Cohort Study. Clinical Kidney Journal, 16(1), 167–175. https://doi.org/10.1093/ckj/sfac210
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2024. All Rights Reserved.

