
OCCUPATIONAL HEALTH AND INJURY RISK PROFILING IN CRICKET WICKETKEEPERS ACROSS COMPETITIVE LEVELS
Sadiya Khan 1![]() , Roopa Rao 2
, Roopa Rao 2![]()
![]()
1 Student,
Department of Community Resource Management, College of Home Science Nirmala
Niketan, (Affiliated to University of Mumbai), Mumbai – 20, Maharashtra, India
2 Associate
Professor, Department of Community Resource Management, College of Home Science
Nirmala Niketan, (Affiliated to University of Mumbai), Mumbai – 20,
Maharashtra, India
|
|
|
ABSTRACT |
|
|
Cricket's
physically demanding nature puts wicketkeepers at high risk for
musculoskeletal injuries, particularly knee strain, lower back pain, and hand
injuries. This study explores the health issues of wicketkeepers through
observational analysis and survey feedback from amateur, professional, and
elite levels. Our research reveals that repetitive squatting, extended
crouching, and sudden lateral movements cause chronic musculoskeletal
disorders (MSDs) due to poor recovery strategies, poor posture, and repetitive
movements. Protective gear like gloves, pads, and footwear plays a crucial
role in reducing injury risks. However, ill-fitting or low-quality equipment
can increase injuries rather than prevent them. Environmental conditions like
uneven or hard playing surfaces and temperature fluctuations also impact
injury prevalence, causing joint stress and muscle fatigue. To promote player
safety and performance, we recommend incorporating strength and conditioning
exercises focused on enhancing flexibility and joint stability. Improved
sports science and biomechanics can create more effective protective
equipment. Implementing preventive strategies into training programs and
equipment design can minimize injury risks, prolong careers, and maximize
performance. This study highlights the significance of evidence-based injury
prevention principles and ergonomic strategies in cricket. Improved ergonomic
equipment design, organized recovery programs, and posture-conscious training
can counteract injury risks. By prioritizing player safety and performance,
cricket can reduce injury prevalence and support the long-term well-being of
wicketkeepers. Our findings have implications for training programs,
equipment design, and safety measures in cricket. By adopting a proactive
approach to injury prevention, wicketkeepers can enjoy longer, healthier
careers, and the sport can benefit from improved player performance and
reduced injury rates. |
|||
|
Received 11 April 2025 Accepted 13 May 2025 Published 03 July 2025 Corresponding Author Sadiya
Khan, sadiyakhan4891@gmail.com DOI 10.29121/granthaalayah.v13.i6.2025.6222 Funding: This study did
not receive financial grants or support from governmental or nongovernmental
funding agencies, cricket boards, or related organizations. Copyright: © 2025 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Wicketkeepers, Musculoskeletal Injuries,
Training Intensity, Protective Gear, Playing Conditions, Cricket Injuries,
Ergonomics |
|||
1. INTRODUCTION
Cricket, a globally celebrated sport, demands a high level of physical, mental, and strategic engagement from its players. Among all fielding positions, wicketkeeping is widely recognized as one of the most physically taxing roles, requiring sustained crouching, explosive agility, and exceptional hand-eye coordination. The wicketkeeper must remain alert throughout the match, frequently performing high-intensity actions such as catching fast deliveries, executing stumpings, and diving laterally to prevent runs. These repetitive actions impose significant biomechanical stress on the lower back, knees, fingers, and shoulders (Stretch, Cricket injuries: A longitudinal study of the nature of injuries to South African cricketers., 2003).
Despite the centrality of this role, the injury profiles and occupational health risks faced by wicketkeepers remain underexplored, especially when compared to the extensive research on bowlers and batsmen Orchard et al. (2002). Prolonged crouching and frequent squatting movements are associated with lumbar stress, patellofemoral pain syndrome, and hamstring tightness. Simultaneously, the abrupt and reactive nature of wicketkeeping contributes to acute injuries such as finger dislocations, wrist sprains, and rotator cuff tears Foster et al. (2018).
Training intensity is another critical determinant of injury. Elite wicketkeepers often undergo rigorous conditioning, including agility drills and reflex training, to enhance performance. However, inadequate rest periods, poor postural conditioning, and insufficient recovery exacerbate the likelihood of overuse injuries Gabbett (2005). Furthermore, variable pitch conditions and weather extremes (e.g., heat-induced dehydration or cold-induced stiffness) affect muscle elasticity, increasing vulnerability to muscle strains and joint injuries Hosea and Hannafin (2012).
Environmental elements, such as playing surface hardness and outfield maintenance, further complicate injury risks. Hard or uneven pitches amplify ball rebound speed, increasing the force transmitted to the hands and forearms during catches, while slippery grounds raise the chances of falls and impact-related trauma Ranson et al. (2008).
While protective gear—gloves, pads, helmets, and footwear—serves as the first line of defense, its effectiveness is contingent upon ergonomic design, fit, and material quality. Studies have shown that ill-fitting or inadequately cushioned gloves contribute to cumulative trauma disorders in the fingers and hands Crisco et al. (2005). Similarly, restrictive leg pads and inappropriate footwear can lead to fatigue and compromised agility, adversely affecting performance and increasing injury risk.
Given the occupational health risks inherent in wicketkeeping, there is a critical need for role-specific injury prevention protocols. Structured strength and flexibility programs focusing on core stability, joint mobility, and neuromuscular control are essential. Additionally, dynamic warm-ups, post- match recovery protocols, and education on the selection and maintenance of protective gear should be standard practice Koutedakis and Sharp (1998).
Despite cricket’s deep-rooted presence in regions such as Mumbai, no comprehensive research has yet targeted the epidemiology of wicketkeeping injuries in such cricket-intensive geographies. This study aims to bridge this critical knowledge gap by providing empirical insights into the injury patterns, game-specific risk factors, and the adequacy of current protective strategies for wicketkeepers across competitive levels.
2. LITERATURE REVIEW
Wicketkeeping in cricket is a physically demanding and high-risk role, characterized by repeated squatting, sudden lateral movements, and high intensity catching, which cumulatively pose considerable risks to musculoskeletal health. Despite its critical role on the field, wicketkeeping has not received proportional academic attention compared to batting and bowling. A growing body of literature now highlights the occupational risks associated with wicketkeeping and the potential preventive strategies that can be employed to mitigate these risks. Injury prevalence among wicketkeepers is significant. A study analyzing injury data in elite Australian cricketers revealed that wicketkeepers contributed 11.6% of all injuries, with hand and finger injuries being the most common Orchard et al. (2002). Hand injuries, including fractures, dislocations, and ligament tears, typically result from direct ball impact or glove-related constraints MacDonald et al. (2013) . In addition to upper extremity injuries, wicketkeepers are prone to lower back pain, patellofemoral issues, and hamstring strains due to prolonged crouching and explosive movements Frost and Chalmers (2014). Musculoskeletal injuries in cricket are closely linked to the intensity of play and player level. A longitudinal study showed higher injury rates in elite players compared to amateurs due to greater training loads and match exposure Nupur and Rao (2023). However, amateur players face unique risks arising from inadequate conditioning, poor playing surfaces, and substandard protective gear Ranson et al. (2008). Thus, analyzing injury trends across different playing levels provides valuable insights into both training-induced injuries and those resulting from infrastructural inadequacies. Game-specific risk factors play a central role in injury causation Rao (2018). Playing surface has emerged as a critical variable, with uneven or excessively hard pitches increasing strain on the knees and spine during squatting Ekegren et al. (2014). Moreover, environmental conditions such as temperature and humidity may contribute to fatigue and delayed reflexes, which heighten the risk of trauma. Incorrect or repetitive movement techniques, especially among less-trained players, amplify biomechanical stress Dennis et al. (2003). The role of protective gear in minimizing injuries has received some attention in sports medicine research. Gloves, pads, and abdominal guards are standard equipment for wicketkeepers, yet studies show that ill-fitting or poor-quality gear often fails to prevent injury. (Stretch, Cricket injuries: A longitudinal study of the nature of injuries to South African cricketers., 2003) noted that even among international players, glove design often did not align with ergonomic standards, leading to compromised shock absorption. Furthermore, local and amateur players often lack access to high-end protective gear, exposing them to higher injury risks. Preventive strategies, including targeted strength and flexibility training, technique correction, and equipment innovations, are advocated by numerous studies. Physiological conditioning focused on core strength and posterior chain mobility has been found to reduce the incidence of lower back and hamstring injuries Gabbett (2005). Additionally, structured wicketkeeping drills that reinforce safe catching and squatting techniques contribute to reducing upper limb trauma. An intervention study emphasized the role of sports science in monitoring workload and tailoring recovery protocols, which could be crucial for injury prevention Dhillon (2012), Rahul and Rao (2022). Comparative studies between playing levels underscore a gap in access to health monitoring and injury management resources. While national and state-level athletes often benefit from physiotherapists and biomechanical analysis, grassroots players typically lack these facilities. This inequity in support systems is a contributing factor to injury mismanagement and recurrence among amateur wicketkeepers Ranson et al. (2008). The literature underscores the complex interplay of biomechanical, environmental, and infrastructural factors that shape the occupational health outcomes of wicketkeepers. Although there is evidence supporting the effectiveness of training and equipment interventions, there remains a significant need for player-specific injury tracking and prevention protocols, especially at lower tiers of play. The present study aims to bridge this knowledge gap by evaluating injury patterns, risk factors, and safety mechanisms in a comprehensive and stratified manner.
3. RATIONALE
Cricket, as one of the most widely played and followed sports globally, involves diverse player roles that demand varying levels of physical and physiological effort. Among these roles, wicketkeeping stands out for its high-intensity physical demands, requiring prolonged crouching, quick reflexes, explosive lateral movements, and frequent catching of high-speed deliveries. These activities expose wicketkeepers to a heightened risk of musculoskeletal disorders (MSDs), including lower back strain, knee and hip discomfort, and hand injuries such as fractures and ligament tears. Despite these risks, research in cricket sports medicine has predominantly focused on batsmen and bowlers, with wicketkeepers remaining an underrepresented group in injury surveillance studies.
This study is justified by the lack of targeted scientific literature addressing occupational health issues specific to wicketkeepers. The combination of biomechanical strain from repetitive postures, acute trauma from high-impact ball catches, and inadequate recovery periods make them vulnerable to both acute and chronic injuries. Additionally, the ergonomic challenges of poorly designed or ill- fitting protective gear exacerbate the risk of injury. Factors such as playing surface hardness, weather conditions, and hydration status further complicate injury mechanisms, particularly in local contexts such as Mumbai, where cricket is played year-round under diverse conditions.
Moreover, training protocols for wicketkeepers are often skill-centric and lack sufficient focus on injury prevention, posture awareness, and recovery. There is minimal integration of physiotherapy, strength conditioning, or equipment optimization tailored to their role. This creates a significant gap in player welfare, especially at amateur and semi-professional levels where access to advanced medical or training support is limited.
Mumbai, often regarded as the cricketing capital of India, has yet to produce city-specific research on the occupational hazards faced by its wicketkeepers. The absence of empirical data on their health outcomes restricts evidence-based policy formulation, training improvements, and ergonomic interventions. By narrowing its scope to this specific role within a distinct cricketing culture, this study seeks to fill an essential gap and provide actionable insights.
Through a detailed investigation into the prevalence, types, and causes of injuries in wicketkeepers across competitive levels, this research aims to propose informed, role-specific prevention strategies. These strategies can lead to improved training methodologies, better-designed protective equipment, and heightened awareness of health maintenance practices. Ultimately, this study is envisioned as a critical contribution to enhancing the safety, performance, and career longevity of wicketkeepers—a vital yet vulnerable category of cricket athletes.
4. AIM AND OBJECTIVES
The primary aim of this study is to assess the occupational health status of cricket wicketkeepers by examining their injury patterns, associated game-specific risk factors, and the effectiveness of protective equipment. The study also seeks to compare injury prevalence and health outcomes across varying levels of play, ranging from amateur to elite cricket, to propose evidence-based injury prevention and safety enhancement strategies. The specific objectives, are to: (i) evaluate the prevalence, nature, and anatomical distribution of injuries sustained by wicketkeepers at different competitive levels (local, district, state, and national); (ii) examine game-specific risk factors— including training volume, playing surface characteristics, wicketkeeping techniques, and the usage of protective equipment—that contribute to occupational injuries and health problems among wicketkeepers; and (iii) assess the adequacy and effectiveness of existing protective gear and training interventions in reducing injury risks and promoting long-term occupational well-being in wicketkeepers.
5. RESEARCH METHODOLOGY
This study employed a descriptive exploratory research design to investigate occupational health risks and injury patterns among cricket wicketkeepers, with particular emphasis on training intensity, playing conditions, and the adequacy of protective equipment. The study aimed to capture a wide spectrum of experiences by recruiting a total of 160 male wicketkeepers across various competitive levels—including amateur, semi-professional, and elite categories—selected from cricket academies, clubs, and organized teams within metropolitan and suburban areas. This ensured the inclusion of players exposed to diverse match environments and training loads. Participants were recruited through a combination of convenience and snowball sampling methods, which enabled the researchers to identify individuals actively engaged in regular cricket training and matches. Clear inclusion criteria required participants to have at least one year of wicketkeeping experience and regular involvement in competitive cricket. Exclusion criteria ruled out individuals with pre-existing severe medical conditions unrelated to cricket or those unwilling to provide informed consent. Data collection involved a multi-method approach to ensure a comprehensive understanding of injury prevalence and contributing risk factors. A self-designed questionnaire captured demographic information, training frequency, playing surface exposure, and protective gear usage. Structured interviews supplemented this data by providing qualitative insights into personal injury experiences, perceptions of equipment effectiveness, and awareness of ergonomic practices. The Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) Hedge (1999) was used to quantify the severity and anatomical distribution of discomfort and injuries. Quantitative data were analyzed using descriptive statistical methods, including frequency distributions and percentage calculations, to identify common trends and risk factors. The influence of contextual variables such as pitch condition, match duration, and environmental stressors was also examined. Ethical protocols were strictly adhered to throughout the research process. All participants provided informed written consent after being briefed on the study’s objectives, and confidentiality was maintained through anonymized data handling. The research upheld principles of voluntary participation, non-coercion, and data protection. This methodological framework ensures the validity and reliability of findings while contributing actionable insights to injury prevention, ergonomic improvements, and performance sustainability for wicketkeepers.
6. RESULTS AND DISCUSSION
6.1. Demographic Profile of the Sample
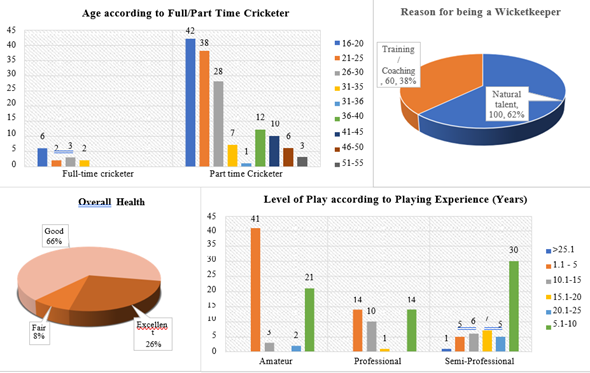
The demographic profile of the study sample on Occupational Health and Injury Risk in Cricket Wicketkeepers offers valuable insights into the diversity and experience distribution of the 160 participants. A significant majority were part-time cricketers, predominantly between the ages of 16 and 30 years, indicating a young and semi- professional player base. In contrast, full-time cricketers were comparatively fewer and largely belonged to the younger age brackets (16–25 years), highlighting a possible transition phase between amateur and professional engagement. The playing experience distribution reveals that amateur players dominate the cohort, especially those with 1–5 years of experience (41 participants). Among semi-professionals, 5.1–10 years of experience was most common, while professional players showed more distributed experience, ranging from 1 to 15 years. This suggests that higher levels of play are associated with broader experience ranges, but relatively fewer participants at elite or prolonged competitive levels. When analyzing the reason for choosing wicketkeeping, 62% cited natural talent, while 38% attributed their skills to training/coaching. This distribution reflects a mix of instinctive ability and structured development, which could influence both performance and susceptibility to injury. In terms of self-assessed overall health, 66% reported good health, 26% excellent, and only 8% fair, indicating a generally healthy population, though possibly underreporting of musculoskeletal discomfort due to perceived athletic norms.
The highlights of the sample are as follows:
· Majority are young, part-time wicketkeepers aged 16–30.
· Amateur level dominates, with most having 1–5 years of experience.
· Natural talent (62%) was more influential than coaching (38%) in wicketkeeper selection.
· Self-reported health was largely good to excellent (92%).
· Professional and semi-professional representation was balanced but lower than that of amateurs, hinting at potential drop-offs due to injury or lack of support.
Figure 1
|
Figure 1 Profile of Sample |
6.2. Injuries Sustained
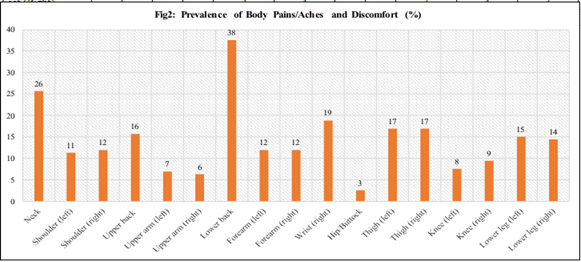
The analysis of the provided data indicates a high prevalence and diverse anatomical distribution of injuries among cricket wicketkeepers across competitive levels. The most common injury types were sprains and strains (39%), followed by muscle tears (30%), fractures (24%), and cuts (5%). Only 1% of participants reported no injury, highlighting the near-universal incidence of physical stress and trauma in this role.
In terms of body regions, the lower back emerged as the most affected site, with 38% of all wicketkeepers reporting discomfort—particularly concentrated among Table 1 semi-professional (25%) and professional (21%) players. Neck pain (26%) and wrist pain (19%) were also prevalent, underscoring the impact of prolonged squatting, repetitive catching, and awkward postures. These results align with previous studies that identify lower back and wrist injuries as highly common in wicketkeepers due to the physical demands of the position.
Interestingly, amateur players reported more diffuse pain across the forearms, thighs, and shoulders, possibly due to inadequate conditioning and limited access to professional recovery protocols Table 1. In contrast, professionals exhibited concentrated discomfort in high-load areas, such as the upper back and right wrist, suggesting overuse associated with more intensive play and repetitive movements.
The data also illustrates the relationship between injury type and preventive strategy. For example, most respondents who experienced sprains and strains (59) cited the need for integrated strategies—encompassing flexibility, strength training, and proper technique—as most effective. In conclusion, the findings highlight a pressing need for targeted injury prevention based on anatomical stress zones and competitive exposure. Strengthening physical preparation and protective strategies could mitigate these common yet avoidable injuries.
Table 1
|
Table 1 Body Sites of Pain/Aches and Discomfort Experiences According to Level of Play |
|||||||||||
|
Body Sites |
Amateur (67) |
Semi-Professional (54) |
Professional (39) |
Total (160) |
|||||||
|
f |
% |
f |
% |
f |
% |
f |
% |
||||
|
Neck |
14 |
21 |
15 |
28 |
12 |
31 |
41 |
26 |
|||
|
Shoulder (Right) |
6 |
9 |
9 |
17 |
4 |
10 |
19 |
12 |
|||
|
Shoulder (Left) |
8 |
12 |
9 |
17 |
1 |
3 |
18 |
11 |
|||
|
Upper Back |
2 |
3 |
7 |
13 |
16 |
41 |
25 |
16 |
|||
|
Upper Arm (Right) |
3 |
4 |
5 |
9 |
3 |
8 |
11 |
7 |
|||
|
Upper Arm (Left) |
4 |
6 |
4 |
7 |
2 |
5 |
10 |
6 |
|||
|
Lower Back |
17 |
25 |
8 |
15 |
9 |
23 |
34 |
21 |
|||
|
Forearm (Right) |
9 |
13 |
5 |
9 |
5 |
13 |
19 |
12 |
|||
|
Forearm (Left) |
7 |
10 |
4 |
7 |
8 |
21 |
19 |
12 |
|||
|
Wrist (Right) |
10 |
15 |
8 |
15 |
12 |
31 |
30 |
19 |
|||
|
Wrist (Left) |
10 |
15 |
8 |
15 |
12 |
31 |
30 |
19 |
|||
|
Hips/Buttocks |
1 |
1 |
3 |
6 |
0 |
0 |
4 |
3 |
|||
|
Thighs (Right) |
12 |
18 |
8 |
15 |
2 |
5 |
22 |
14 |
|||
|
Thighs (Left) |
14 |
21 |
9 |
17 |
4 |
10 |
27 |
17 |
|||
|
Knee (Right) |
9 |
13 |
5 |
9 |
1 |
3 |
15 |
9 |
|||
|
Knee (Left) |
4 |
6 |
7 |
13 |
1 |
3 |
12 |
8 |
|||
|
Lower Leg (Right) |
5 |
7 |
14 |
26 |
4 |
10 |
23 |
14 |
|||
|
Lower Leg (Left) |
6 |
9 |
11 |
20 |
6 |
15 |
23 |
14 |
|||
|
Feet (Right) |
1 |
1 |
2 |
4 |
1 |
3 |
4 |
3 |
|||
|
Feet (Left) |
1 |
1 |
2 |
4 |
2 |
5 |
5 |
3 |
|||
Figure 2
|
Figure 2 Prevalence of Body Pains/Aches and Discomfort (%) |
6.3. Game-Specific Risk Factors Contributing to Occupational Injuries
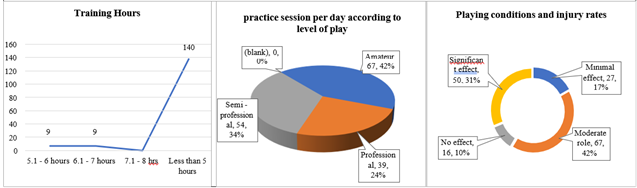
Results illustrate several game-specific factors contributing to injury risk among wicketkeepers. Training volume appears moderate across most respondents—140 participants report less than 5 hours of daily training, suggesting insufficient volume for conditioning Figure 3. This undertraining could result in muscle fatigue and poor injury resilience, especially given that most practice sessions are weekly (58%) or monthly (16%), and only 16% engage in daily training. Furthermore, 92% of participants are part-time cricketers Figure 3, indicating inconsistent exposure to professional-level conditioning programs.
Figure 3
|
Figure 3 Game-Specific Risk Factors Contributing to Occupational Injuries |
Environmental conditions also play a notable role: 42% of respondents agree that playing conditions have a moderate effect, while 31% report a significant effect on injury rates Figure 3. Factors like hard or uneven pitches, poor weather, and inadequate drainage likely contribute to sprains, strains, and overuse injuries, especially during matches with extended durations.
Table 1
|
Table 1 Body Sites of Pain/Aches and Discomfort Experiences According to Level of Play |
|||||||||||
|
Body Sites |
Amateur (67) |
Semi-Professional (54) |
Professional (39) |
Total (160) |
|||||||
|
f |
% |
f |
% |
f |
% |
f |
% |
||||
|
Neck |
14 |
21 |
15 |
28 |
12 |
31 |
41 |
26 |
|||
|
Shoulder (Right) |
6 |
9 |
9 |
17 |
4 |
10 |
19 |
12 |
|||
|
Shoulder (Left) |
8 |
12 |
9 |
17 |
1 |
3 |
18 |
11 |
|||
|
Upper Back |
2 |
3 |
7 |
13 |
16 |
41 |
25 |
16 |
|||
|
Upper Arm (Right) |
3 |
4 |
5 |
9 |
3 |
8 |
11 |
7 |
|||
|
Upper Arm (Left) |
4 |
6 |
4 |
7 |
2 |
5 |
10 |
6 |
|||
|
Lower Back |
17 |
25 |
8 |
15 |
9 |
23 |
34 |
21 |
|||
|
Forearm (Right) |
9 |
13 |
5 |
9 |
5 |
13 |
19 |
12 |
|||
|
Forearm (Left) |
7 |
10 |
4 |
7 |
8 |
21 |
19 |
12 |
|||
|
Wrist (Right) |
10 |
15 |
8 |
15 |
12 |
31 |
30 |
19 |
|||
|
Wrist (Left) |
10 |
15 |
8 |
15 |
12 |
31 |
30 |
19 |
|||
|
Hips/Buttocks |
1 |
1 |
3 |
6 |
0 |
0 |
4 |
3 |
|||
|
Thighs (Right) |
12 |
18 |
8 |
15 |
2 |
5 |
22 |
14 |
|||
|
Thighs (Left) |
14 |
21 |
9 |
17 |
4 |
10 |
27 |
17 |
|||
|
Knee (Right) |
9 |
13 |
5 |
9 |
1 |
3 |
15 |
9 |
|||
|
Knee (Left) |
4 |
6 |
7 |
13 |
1 |
3 |
12 |
8 |
|||
|
Lower Leg (Right) |
5 |
7 |
14 |
26 |
4 |
10 |
23 |
14 |
|||
|
Lower Leg (Left) |
6 |
9 |
11 |
20 |
6 |
15 |
23 |
14 |
|||
|
Feet (Right) |
1 |
1 |
2 |
4 |
1 |
3 |
4 |
3 |
|||
|
Feet (Left) |
1 |
1 |
2 |
4 |
2 |
5 |
5 |
3 |
|||
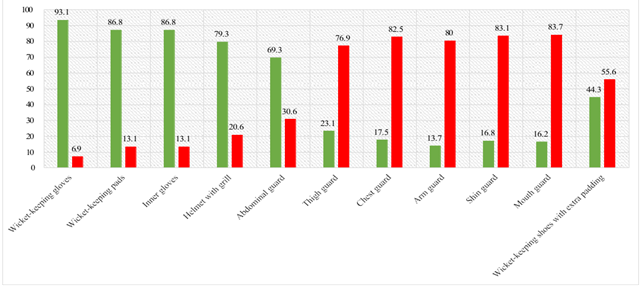
Finally, usage of protective gear shows that while gloves, pads, and helmets are widely adopted (above 79%), low uptake is observed for crucial injury-preventive gear like chest guards (17.5%), arm guards (13.7%), shin guards (16.8%), and wicketkeeping shoes (44.3%) Table 2. Inadequate protective coverage across vulnerable body parts exposes wicketkeepers to both impact and overuse injuries, particularly in amateur and semi-professional play where equipment access may be limited.
6.4. Effectiveness of Protective Gear and Training Interventions
54% of players feel that protective gear significantly reduces injury incidence, while 21% observe moderate benefits. However, 13% report no impact, likely due to improper fit, low usage rates of complete gear sets, or outdated equipment. Although 69% always use protective gear, 31% either do not use it consistently or opt out altogether, posing a major risk to injury prevention efforts.
Training adequacy also remains questionable. Only 16% of respondents train daily, and nearly all train less than 5 hours a day. This low volume of sport-specific physical preparation may compromise neuromuscular conditioning and joint protection. Additionally, poor implementation of recovery protocols could worsen cumulative stress, especially on high-load anatomical zones like the lower back, knees, and wrists. Hence, while existing protective measures do reduce injuries, their effectiveness is undermined by inconsistent usage, lack of full-body coverage, and inadequate training interventions. For effective injury mitigation, comprehensive ergonomic education, conditioning routines, and personalized gear fitting are essential.
Figure 4
|
Figure 4 Use of Protective Gear |
7. RECOMMENDATIONS AND ERGONOMIC REMEDIES FOR PREVENTING CVS AND WORK-RELATED MUSCULOSKELETAL DISORDERS
Maintaining player safety, performance, and health in sports needs a multi-tiered approach of players, coaches, government officials, and enforcers of the policy. On the player level, players need to continually wear protective equipment like helmets, thigh guards, and chest guards to reduce the risk of injury. In addition, attention to physical fitness, injury precaution skills, and suitable nutrition is crucial for enhancing performance and longevity in their sports careers.
Targeted ergonomic and biomechanical interventions across four key domains:
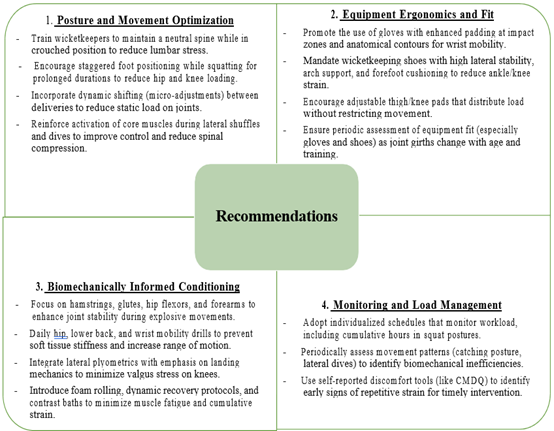
These recommendations should be implemented in wicketkeeper-specific injury prevention programs, co-developed with physiotherapists, sports scientists, and equipment designers to reduce injury risk and support long-term occupational health.
CONFLICT OF INTERESTS
The authors disclose that they have no conflicting interests that could potentially influence the objectivity or integrity of the research conducted.
Informed Consent
Before their participation, all participants provided written informed consent, demonstrating their understanding of the study’s objectives, procedures, and potential risks.
ACKNOWLEDGMENTS
The researchers express their sincere gratitude to the wicketkeepers who participated in this study, including amateur, professional, and elite players, for their valuable contributions and insights.
REFERENCES
Crisco, J. J., Greenwald, R. M., & Chou, P. H.
(2005). Finger Injury
Risks in Sport: Glove
Performance and Biomechanics. Clinical
Journal of Sport Medicine, 15(2), 114–121.
Dennis, R., Farhart,
P., Goumas, C., & Orchard, J. (2003). The Reliability of Musculoskeletal
Screening Tests used in Cricket. Physical Therapy in Sport, 4(1), 25–33.
Dhillon, M. S. (2012). Epidemiology of Orthopedic
Injuries in Indian Cricket:
A Prospective One Year Observational
Study. [Journal Name Missing].
Ekegren, C. L., Gabbe, B. J., Donaldson, A., & Finch, C. F. (2014). Injuries in Community-Level Australian Football: Results from a Club-Based Injury Surveillance Program. Journal of Science and Medicine in Sport, 19(2), 150–157.
Foster, D., John, D., & Kelly, M. (2018). Injury Surveillance in Elite Cricket: A Review of Current Findings and Future Directions. British Journal of Sports Medicine, 52(4), 223–228.
Frost, W. L., & Chalmers, D. J. (2014). Injury in Elite New Zealand Cricketers 2002–2008: Descriptive Epidemiology. British Journal of Sports Medicine, 48(12), 1002–1007. https://doi.org/10.1136/bjsports-2012-091337
Gabbett, T. J. (2005). Science of Rugby League Football: A Review. Journal of Sports Sciences, 23(9), 961–976. https://doi.org/10.1080/02640410400023381
Hedge, A. (1999). CU Ergo – Cornell University Ergonomics Web: Cornell Modified Discomfort Questionnaire (CMDQ). Cornell University. https://doi.org/10.1037/t60061-000
Hosea, T. M., & Hannafin, J. A. (2012). Sports-Specific Injuries: Upper Extremity. Clinics in Sports Medicine, 31(2), 331–352.
Koutedakis, Y., & Sharp, N. C. (1998). The Fit and Healthy Dancer. Journal of Dance Medicine & Science, 2(3), 65–71. https://doi.org/10.1177/1089313X9800200203
MacDonald, D., Cronin, J., Mills, J., & Stretch, R. (2013). Wicket-Keeping in Cricket: A Literature Review. International Journal of Sports Science & Coaching, 8(3), 336–339. https://doi.org/10.1260/1747-9541.8.3.531
Nupur, S., & Rao, R. (2023). Awareness About Protective Devices Among Basketball Players (Aged 20–30 Years). International Journal of Multidisciplinary
Education Research, 13(5), 82–86.
Orchard, J., James, T., Kountouris, A., & Portus, M. (2002). Fast Bowling Match Workloads Over 5–26 Days
and Risk of Injury in the following
Month. Journal of Science and Medicine
in Sport, 15(6), 493–497.
Rahul, P., & Rao, R. (2022). Intake of Nutritional Supplements Among People Who Frequently Exercise at Gyms. International Journal of Multidisciplinary Educational Research, 11(12), 26–34.
Ranson, C., Burnett, A., King, M., Patel, N., & O'Sullivan, P. (2008). The Relationship Between Cricket Fast Bowling Technique and Back Injury. Journal of Sports Sciences, 26(8), 887–897. https://doi.org/10.1080/02640410701501671
Rao, R. (2018). Introduction to Ergonomics. Mumbai: [Publisher not Listed].
ISBN 978-93-5321-4500.
Stretch, R. A. (2001). The Incidence and Nature of Injuries in First-League and Provincial Cricketers. South African Medical Journal, 91(4), 336–339.
Stretch, R. A. (2003). Cricket Injuries: A Longitudinal Study of the Nature of Injuries to South African Cricketers. British Journal of Sports Medicine, 37(3), 250–253. https://doi.org/10.1136/bjsm.37.3.250
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2025. All Rights Reserved.

