
Toxicity (Toxic material) score and Cocktail treatments (Covi Wonder) for Long Covid: A retrospective cohort study
Ki-Yeob Jeon 1![]()
![]()
1 MD,
Jeonbuk National University, ROK; PhD, Chonnam National University, ROK; ScD,
Johns Hopkins University, USA
|
|
|
ABSTRACT |
|
|
Introduction: A long Covid represents systemic, disabling conditions of more than three months that associated with acute SARS-CoV-2 infections or post-acute sequelae of Covid (PASC). It can be diagnosed on clinical bases without a definite diagnostic tool nor a treatment. The study was done to evaluate both the toxicity score of the blood for the diagnosis of and the Cocktail medication for the healing of long Covid. Methods: Among patients who visited our clinic from June 2022 to January 2025, 48 patients with long Covid-19 finished all the series of peripheral blood smear, blood chemistry and blood toxicology tests more than twice. While 10 patients did not have cocktail medications to treat their long Covid, 38 patients were treated by the recommended protocols including Cocktail medications of our clinic. Among 38 patients, one outlier, who showed familial allergic reactions to PEG (polyethylene glycol) was removed from the Wilcoxon matched paired t tests. Results: The mean age of the untreated 10 patients was 59.7 ± 9.55 years old and that of treated 37 patients was 56.1 ± 13.61 years. Untreated patients with Cocktail medication showed minimal improvements of their previous symptoms in the following visits, and the toxicity score of the blood increased significantly from 12.90 ± 7.20 to 18.30 ± 5.25 (Wilcoxon test: z = - 2.536, p= 0.011). Treated 37 patients with cocktail medication showed significant symptomatic improvements in their follow-up visits and the toxicity score of the blood significantly decreased from 12.92 ± 5.18 to 7.76 ± 2.99 (Wilcoxon Test: z = - 4.783, p < 0.001). Conclusion: The results show that the toxicity (toxic material) score of the
blood can be a diagnostic tool for and the Cocktail
medications can be a healing protocol for the long Covid. |
|||
|
Received 19 March 2025 Accepted 22 April 2025 Published 07 June 2025 Corresponding Author Ki-Yeob
Jeon, kjeon@hanmail.net DOI 10.29121/granthaalayah.v13.i5.2025.6166 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2025 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: COVID-19 Injectables, Healing Protocols,
Long COVID Syndrome, Shedding, Toxicity Score, Toxicology Test, Cocktail
Treatment (Covi Wonder), Healing Protocol, Graphene Oxide, Polyacrylamide
Hydrogel, Microchips |
|||
1. INTRODUCTION
Long Covid was defined by seven different committees, including U.S. CDC 2020, U.K. NICE 2020, U.S. DASH 2022, WHO Adults 2022, WHO Children 2022, U.S. RECOVER 2023, and NASEM 2024. Ely et al. (2024) It is a chronic status with single or multiple symptoms or conditions lasting at least 3 months following a confirmed, probable, or possible SARS-CoV-2 infection. There are many people who complain fatigability, exertional dyspnea and palpitation, and brain fog, It affects a wide-range of people (10-30% of non-hospitalized and 50-70% of hospitalized SARS-CoV-2 cases, and 10-12% Covid vaccinated cases). Hadanny et al. (2024) It was reported that more than 60 million people globally (7% adults and 1% children in the United States) were affected by long Covid. Ely et al. (2024) Based on the previous research that the toxicity score (toxicology test) of the blood is a diagnostic tool and the Cocktail medications is a healing protocol for the sequelae of Covid-19 vaccination Jeon (2024), the current study hopes to expand and apply the current usage of toxicity score (toxicology test) of the blood and the Cocktail medications to the diagnosis and healing for the long Covid.
2. Method
Among patients who visited our clinic from June 2022 to January 2025, 1,101 patients were interviewed and had the blood tests for the treatments and status evaluations of their long Covid. Among them, 48 patients finished all the series of peripheral blood smear, blood chemistry and toxicology tests more than twice. While 10 patients did not have Cocktail medications to treat their long Covid, 38 patients were treated by the recommended protocols of Cocktail medications (Covi Wonder) of our clinic as seen in the previous article. Jeon (2024) Our clinic recommended taking Cocktail medications at least for 5 months and 10 days. For the first 10 days, people were prescribed in our clinic Azithromycin, Montelukast, Cetirizine, Gingko biloba, Vitamin C & D & zinc, Acetylcysteine, Hydroxychloroquine, Omega-3, Fenofibrate, Artemisinin, Melatonin, Ivermectin, fermented soybeans (Hamssine Cheonggukjang™), Smart-Food-DM™ (Mixed powder of Houttuynia cordata, Green Tea, Mulberry leaves, Licorice, and Coix agretis), and Naltrexone. And for the later 5 months, Montelukast, Fexofenadine, Hydroxychloroquine, Aspirin, Gingko biloba, Acetylcysteine, Vitamin C & D & zinc, Melatonin, Fenofibrate, Ivermectin, Naltrexone, Bromelain, Artemisinin, fermented soybeans (Hamssine Cheonggukjang™), MMS2 (calcium hypochlorite), and Smart-Food-DM ™ were prescribed. Everyone, who took either 10-day Cocktail medications or 10-day Cocktail medications and on-going 5-month Cocktail medications, was included in the treatment group of Cocktail medication. Only small portion of treated people (about 10 among 38 people) took artemisinin, MMS2, Hamssine Cheonggukjang, ™ or Smart-Food-DM™. Some who were allergic to any specific medications such as aspirin, hydroxychloroquine, ivermectin, or fenofibrate, did not take the specific allergic medication. But only those patients who finished all the necessary studies, which are peripheral blood smear, blood chemistry and blood toxicology tests, were included in the data analysis. One outlier among 38 patients, who showed familial allergic reactions to PEG (polyethylene glycol), was eliminated from the Wilcoxon matched paired t tests of the IBM SPSS statistics™.
Toxicity (toxic material) score in the blood was tested as seen in the previous article, however, the criteria were a little modified in this article, as seen in the Table 1 Toxic materials were observed separately both in the peripheral blood and in the centrifuged plasma. The toxic material (especially, graphene oxide or polyacrylamide hydrogel filaments or ribbons) of the peripheral blood was observed and scored separately and independently. When Graphene oxide (GO)-like materials were found in the peripheral blood, all the findings in the centrifuged plasma were disrespected, and only final score of 22 or 20 was given (22 if the size of primary graphene oxide is larger than 150 micrometer, and 20 if its size is less than 149 micrometers). If a graphene oxide-like material is absent in the peripheral blood smear, the toxic material score of the centrifuged (for 30-minutes with 2200 rpm) plasma was assigned according to the stereomicroscopic observations of the previous study. The toxicity (toxic material) score for each item in the centrifuged plasma was added into the total toxicity score as seen in the Table 1 The highest possible total score is 24, which is the severest form in the blood toxicity test, and the lowest one is 0 (zero) which may be impossible to get in a contaminated world where everybody lives. There are six categories of the toxic items in the plasma toxicology tests: total size of graphene oxide-like material (polyacrylamide hydrogel filaments or ribbons) / microchip (4 points for over 300 micrometers, 3 points for over 100 to 299, 2 points for over 50 to 99, 1 point for 1 to 49, 0 points for no GO/microchip); total size of dough-like inflammatory mass (4 points for over 300 micrometers, 3 points for 100-299, 2 points for 50-99, 1 point for 1-49, 0 points for no inflammatory mass); number of actively moving microrobots (4 points for over 7 particles, 3 points for 4-6, 2 points for 2-3, 1 point for 1, 0 for no particle); number of inflammatory cells (4 points for over the slide surface; 3 points for 3/4 of the slide, 2 points for 1/2 of the slide, 1 point for 1/4 of the slide, 0 points for scarce inflammatory cells), number of crenated red blood cells (RBCs) (4 points for over 20, 3 points for 10-19, 2 points for 5-9, 1 point for 1-5, 0 for 0), and number of RBC rouleau (4 points for over 20 or large, 3 points for 10-19 or medium, 2 points for 5-9 or moderate, 1 point for 1-4 or slight, 0 points for 0).
Table 2 shows that there are five categories of toxic material content or toxicity severity in the blood according to the total score of the sum of the 7 sub-scores: very severe for over 20 points of the 24 total points, severe for 15-19, moderate for 9-14, mild for 4-8, and slight for 0-3.
Table 1
|
Table 1 A summarized table ofthe toxicity (toxic material) score. This is a modified Table from the previous study. Jeon (2024) Toxic materials in the peripheral blood and toxic material score of the centrifuged plasma was assigned according to the stereomicroscopic observations. In the peripheral blood, a graphene oxide or polyacrylamide hydrogel filament or ribbon was mainly observed and scored as 22 or 20. In the centrifuged plasma, six items (total size of Graphene Oxide-like material, total size of dough-like inflammatory mass, number of actively moving microrobots, number of inflammatory cells, number of crenated red blood cells [RBCs]), and number of RBC rouleaux) were observed and scored accordingly. |
|||||
|
Toxic | material | Sub-Score Item | |
4 |
3 |
2 |
1 |
0 |
|
1. Number and/or size
of secondary graphene oxide-like material |
300≥x |
300>x≥200 |
200>x≥100 |
100>x≥1 |
0 |
|
2. Number and/or size
of dough-like mound structures |
300≥x |
300>x≥200 |
200>x≥100 |
100>x≥1 |
0 |
|
3. Number aand/or size of inflammatory cells |
3/4≥x |
2/4≥x |
1/4≥x |
x≥1/10 |
0 |
|
4. Number of moving Microrobots |
10≥x |
10>x≥7 |
7>x≥4 |
4>x≥1 |
0 |
|
5. Number of
crenated/damaged red blood cells (echinocytes) |
30≥ |
30>x≥20 |
20>x≥10 |
10>x≥1 |
0 |
|
6. Number and/or size
of red blood cell (RBC) rouleaux |
30≥ |
30>x≥20 |
20>x≥10 |
10>x≥1 |
0 |
|
7. Number and/or size
of primary Graphene Oxide (or polyacrylamide hydrogel filament/ ribbon/
polymers) and other toxic materials in the peripheral blood slide |
The total score is 22
(very severe) if the size of primary graphene oxide is larger than 150
micrometer, and 20 (severe) if its size is less than 149 micrometers. If a
graphene oxide is absent in the peripheral blood smear, other toxic
materials were evaluated and scored as those in the plasma. |
||||
Table 2
|
Table 2 Five categories of the toxicology (Toxicity severity) test in the blood according to the total score of blood toxicity (toxic material) score as seen in the previous study. There are five categories of toxic material contents or toxicity severity of the blood according to the total score of the sum of the 7 sub-scores: very severe for over 20 points of the 24 total points, severe for 15-19, moderate for 9-14, mild for 4-8, and slight for 0-3. |
|
|
Very Severe |
X ≥ 20 |
|
Severe |
19≥x≥15 |
|
Moderate |
14≥x≥9 |
|
Mild |
8≥x≥4 |
|
Slight |
3≥x≥0 |
3. Results
Those who did not receive Cocktail treatments comprised 10 individuals, with a mean age of 59.7 ± 9.55 years; the youngest participant was 43 years old, while the oldest one was 71 years old. In contrast, those who had Cocktail treatments were 38 individuals, but one outlier was excluded from the final data analysis of the Wilcoxon test. The mean age of the remaining 37 individulas was 56.1 ± 13.61 years, with the youngest being 24 years old and the oldest 81 years old. Among 37 individulas, 14 people were male, 23 were female, and 27 had Covid-19 vaccination at least one time and 10 people had not been vaccinated at all.
Blood chemistry tests conducted on the untreated ten individuals primarily revealed Vitamin D deficiency, decreased hemoglobin levels, decreased white blood cell counts, decreased red blood cell counts, and pancreatic enzyme elevation. The initial blood tests of the untreated showed following results: no D-dimer elevation (0/10), Vitamin D deficiency (7/10), decreased white blood cells (4/10), decreased red blood cells (4/10), decreased hemoglobin (6/10), increased monocytes (1/10), no abnormal thyroid function tests (0/10), elevated CPK-MB (1/10), elevated pancreatic enzyme (2/10), no elevation of lipids (0/10), no elevation of blood glucose (0/10), and no positive CRP (0/10). The follow up blood tests showed: no D-dimer elevation (0/10), Vitamin D deficiency (5/10), decreased white blood cells (7/10), decreased red blood cells (7/10), decreased hemoglobin (7/10), increased monocyte (3/10), abnormal thyroid function tests (3/10), elevated CPK-MB (2/10), elevated pancreatic enzyme (5/10), no elevation of lipids (0/10), no elevation of blood glucose (0/10), and two positive CRPs (2/10).
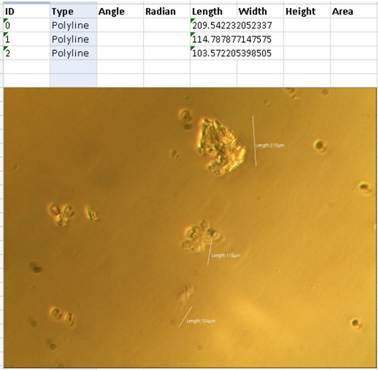
The symptoms and conditions of the treated 38 individuals at the beginning (pre-treatment) was very broad and diverse. The common symptoms included: brain fog, headache, and/or decreased memory (23 out of 38, 60.5%), tinnitus and/dizziness (11/38, 28.9%), a sudden decrease in visual acuity (6/38, 15.8%), chest pain and/or chest tightness (20/38, 52.6%), intermittent chronic coughing and/or intermittent dyspnea (11/38, 28.9%), tiredness and/or fatigability and/or lethargy (25/38, 65.8%), indigestion and/or intermittent abdominal pain (17/38, 44.7%), arthritis and/or myalgia (11/38, 28.9%), skin trouble and/or itching and/or creeping sensation (9/38, 23.7%), herpes and/or vesicle formation (4/38, 10.5%), coldness and/or numbness in the extremities (13/38, 34.2%), unnoticed sudden petechias (9/38, 23.7%), limited motion and/or intermittent paresis (8/38, 21.1%), back pain and/or damaged intervertebral disc (9/38, 23.7%), insomnia and/or sleeping difficulty (19/38, 50%), depression, phobia, and/or aggressive personality (13/38, 34.2%), indifferent and unsensitive feelings and alienation to one’s environments (3/38, 7.9%).
Blood chemistry tests conducted before the treatment of the treated 38 individuals (when they started to treat their long Covid) showed following results: D-dimer elevation (5 out of 38, 13.2%); vitamin D deficiency (19/38, 50%); decreased white blood cell counts (8/38, 21.1%); decreased red blood cell counts (8/38, 21.1%); decreased hemoglobin levels (5/38, 13.2%); increased monocytes (2/38, 5.3%); abnormal thyroid function tests (10/38, 26.3%); elevated CPK-MB (3/38, 7.9%); elevated pancreatic enzymes (4/38, 10.5%); elevation of lipid levels (13/38, 34.2%); elevated glucose levels (5/38, 13.2%); and positive CRPs (2/38, 5.3%). Their follow up blood tests conducted during the treatment indicated: D-dimer elevation (11/38, 28.9%); vitamin D deficiency (9/38, 23.7%), decreased white blood cell counts (11/38, 28.9%), decreased red blood cell counts (13/38, 34.2%), decreased hemoglobin levels (9/38, 23.7%), increased monocyte (5/38, 13.2%), abnormal thyroid function tests (8/38, 21.1%), elevated CPK-MB (1/38, 2.6%), elevated pancreatic enzymes (5/38, 13.2%), elevated lipid levels (11/38, 28.9%), elevated glucose levels (5/38, 13.2%), and positive CRPs (1/38, 2.6%).
Data analyses were conducted using the Wilcoxon matched paired T test with SPSS™. Blood toxicity scores (indicating the presence of toxic materials in the blood) of the untreated 10 individuals showed significantly elevated or aggravated levels of toxic blood tests. At first, the distribution of the blood toxicity levels of the untreated 10 individuals revealed a biphasic one, exhibiting two peaks at the severe and at the mild stages: very severe (2 out of 10, 20%); severe (4/10, 40%): moderate (0/10); mild (3/10, 30%); and slight (1/10, 10%). The mean toxic score of the blood was 12.90 ± 7.20. The follow-up study of the 10 untreated individuals showed a skewed distribution to the very severe and the severe stages: very severe (6 out of 10, 60%), severe (3/10, 30%), moderate (0/10), mild (1/10, 10%), slight (0/10). The follow-up mean toxic score of the untreated 10 individuals was 18.30 ± 5.25, indicating a significant increase, which meant there were more accumulation of toxic materials and more inflammatory processes in the untreated 10 individuals than those at the initial assessment. (Wilcoxon test: z = - 2.536, p= 0.011). The toxicity score of the treated 37 individuals demonstrated significant decrease or improvement in the blood toxicity after Cocktail treatment for the long Covid. At first, before the Cocktail treatment, they showed a balanced distribution as follows: very severe (6/37, 16.2%), severe (10/37, 27.0%), moderate (13/37, 35.1%), mild (8/37, 21.6%), and slight (0/37). The initial mean of their toxicity (toxic material) score was 12.92 ± 5.18. Follow-up study of the 37 treated people showed a dramatically improved distribution of toxicity levels as follows: very severe (0/37), severe (2/37, 5.4%), moderate (9/37, 24.3%), mild (25/37, 67.6%), and slight (1/37, 2.7%). The follow-up mean toxicity (toxic material) score of the treated 37 individuals was 7.76 ± 2.99, indicating a significant decrease, which meant there were much less accumulation of toxic materials and much less inflammatory processes in the treated 37 individuals than those at the beginning. (Wilcoxon Test: z = - 4.783, p < 0.001) Table 3
Table 3
|
Table 3 Blood
toxicity, defined as the presence of toxic materials in the blood, scores of
both the untreated 10 individuals and the treated 37 individuals. Data
analyses were conducted using the Wilcoxon matched paired T test with SPSS™.
The mean ages of the two groups were 59.7 ± 9.55 years for the untreated
group and 56.1 ± 13.61 years for the treated groups, respectably. In the
untreated 10 individuals, the initial mean blood toxicity score was 12.90 ±
7.20, while the follow-up mean toxicity score
increased to 18.30 ± 5.25. There was a significant (p < 0.05) more
accumulation of toxic materials and more inflammatory processes in the
untreated 10 individuals than those at the beginning. (Wilcoxon test: z = -
2.536, p= 0.011). In the treated group of 37 individuals, the mean of their
toxicity (toxic material) score before the treatment was 12.92 ± 5.18 and the
follow-up mean toxicity (toxic material) score decreased to 7.76 ± 2.99,
There were much less accumulation of toxic materials and much less inflammatory
processes in the treated 37 individuals compared to the baseline of the
beginning. (Wilcoxon Test: z = -
4.783, p < 0.001) |
||||
|
Mean of Toxic Material
Score in the blood |
||||
|
Untreated (N= 10) |
Treated (n = 37) |
|||
|
Before |
After |
Before |
After |
|
|
Wilxoxon matched paired T test of the Vaccinated |
13.00 ± 7.90 |
17.57 ± 6.19 |
11.89 ± 4.36 |
8.00 ± 3.20 |
|
z = - 2.032 p = 0.042 |
z = - 3.94 p < 0.001 |
|||
|
Wilxoxon matched paired T test of the Unvaccinated |
12.67 ± 6.81 |
20.00 ± 1.73 |
15.70 ± 6.39 |
7.70 ± 3.20 |
|
z = - 1.60 p = 0.109 |
z = - 2.50 p = 0.013 |
|||
|
Wilxoxon matched paired T test of the Total |
12.90 ± 7.20 |
18.30 ± 5.25 |
12.92 ± 5.18 |
7.76 ± 2.99 |
|
z = - 2.536, p= 0.011 |
z = - 4.783, p < 0.001 |
|||
|
Mean Age |
59.7 ± 9.55 |
56.1 ± 13.61 |
||
Case Vignettes: Three representative examples
Patient 1: A 53-year-old female received two doses of the Covid-19 vaccine and subsequently experienced SARS-CoV-2 infection once after the vaccinations. She had coughing for the past three weeks, was unable to eat due tof nausea, and became lethargy, resulting in a significant loss of her mental power and physical energy. Additionally, she had brain fog, chest tightness, and had difficulty in climbing on the stairs. She did not have herpes, skin troubles, arthritis, depression, loss of her feelings, tinnitus, or visual acuity loss. Her laboratory results indicated a d-Dimer level of 0.33 mg/L, glucose 101 mg/dL,, HA1C 6.2%, Hemoglobin 11.3 g/dL, red blood cell counts 3.61 million/μL, T4 0.89 ng/dL, TSH 8.71 μIU/mL, CK-MB 13.10 ng/mL (normal range: 0-3.61) and Troponin 4.073 ng/mL (normal range: 0-0.3). Pre-treatment blood toxicology test yielded a total score of 6. Figure 1
After 15 days of Cocktail treatment, her symptoms had almost subsided although she continured to experience weakness and a loss of strength. Her blood chemistry tests returned to normal: a d-Dimer level of 0.27 mg/L, glucose 101 mg/dL,, HA1C 6.1%, Hemoglobin 13.3 g/dL, red blood cells 4.27 million/μL, T4 1.09 ng/dL, TSH 5.57 μIU/mL, CK-MB 1.84 ng/mL (normal range: 0-3.61) and Troponin 0.004 ng/mL (normal range: 0-0.3). Follow-up blood toxicology test yielded a total score of 4. Figure 2 and Figure 3
Figure 1
|
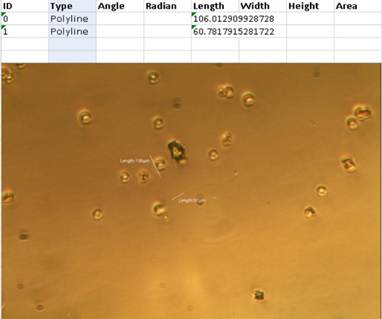
Figure 1 Stereomicroscopic features (pre-treatment) of a 53-year-old female patient who exhibited elevated CK-MB levels and probable myocardial injury. Toxicology test revealed no presence of Graphene Oxide-like materials (polyacrylamide hydrogel filaments or ribbons) or microchips in the peripheral blood. The toxicology test of the plasma showed a 106 micrometer graphene-like material (point 2), no-dough, few inflammatory cells (point 1), a few microrobots (point 1), several crenated red blood cells (RBCs) (point 2), and no RBC rouleaux, which is a total score of 6. |
Figure 2
|
Figure 2 Stereomicroscopic Feature (after Treatment) of a 53-year-old Female who is Recovering from a High CK-MB and Probable Myocardial Injury |
Figure 3
|
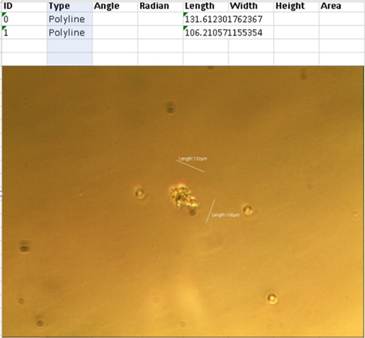
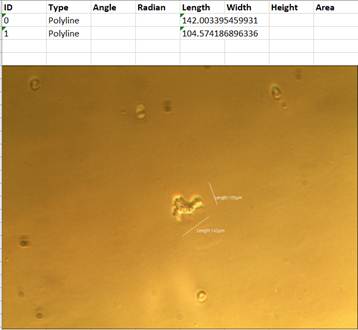
Figure 3 Stereomicroscopic features (post-treatment) of a 53-year-old female patient who is recovering from an elevated CK-MB levels and probable myocardial injury. Toxicology test revealed no presence of Graphene Oxide-like materials (polyacrylamide hydrogel filaments or ribbons) or microchips in the peripheral blood. Toxicology test of the plasma revealed a 131 micrometer graphene-like material (point 2), and 142 micrometer dough-like inflammatory cells (point 2), with no inflammatory cells, no microrobots, no crenated red blood cells (RBCs), and no RBC rouleaux observed, resulting in a total score of 4. |
Patient 2: A 61-year-old female patient who was treated at several hospitals in Los Angeles and Las Vegas, U.S.A., for her abdominal pain, herpes zoster-like vesicles that produced black-colored bloody discharges, and felt worms creeping under her skin and moving within her body. She was vaccinated once with Johnson & Johnson Covid-19 vaccine. She did not remember to have any SARS-CoV-2 infection. She has no history of diabetes mellitus or hypertension. After being informed that no further treatment was avalable in the U.S.A., she came to South Korea and visited multiple hospitals for 2 month period without success. During this time, metal or metal pin-like materials were found in her clotted blood through cupping methods used in Oriental medicine. Figure 5 and Figure 6 She came to our clinic with insomnia, tinnitus in both ears and dizziness, headache and weakened visual acuity, brain fog, chronic persistent coughing, chest tightness, fatigability, abdominal bloating and indigestion, generalized arthralgia, coldness of the extremities, creeping sensations under the skin, skin herpes-like vesicles that produced black-colored bodily discharges, depressive feeling and phobia, severe backpain, and because she felt she would die in the near future and wanted to visit South Korea before she die. Her blood chemistry on her first visiting (October 29, 2024) showed elevated d-Dimer level (0.85 > 0.50 mg/L), elevated platelets (450 > 400 hundred/microL), elevated eosinophil (16.9% > 6%). elevated aspartate transaminase and alanine transaminase (AST 70>40, ALT 68>25 mg/dL), elevated thyroid-stimulating hormone (TSH 4.94> 4.20 μIU/mL), and all the others including HA1C, white and red blood cell counts, homogloin, hematocrit, cholesterol, triglyceride, CK-MB, Troponin, HIV test, lipase and amylase, creatinine and BUN were normal. Pre-treatment blood toxicology test showed total score of 8. Figure 4
The patient was admitted to our clinic and was treated by Cocktail medications and intravenous injections for 10 days, following the healing protocols described in the previous article.[3] Her follow-up blood test on November 8, 2024 (10 days after the Cocktail treatment), showed normal d-Dimer levels (0.42 < 0.5 mg/L), elevated platelets (439 > 400 hundreads/ μL), elevated eosinophils (12.1 > 6.0 %), and elevated AST (71 > 40 IU/L), but normal ALT and normal TSH level. Follow-up blood toxicology test yielded total score of 7. Figure 7 She felt significantly relieved from her symptoms; however, she had to return to her home in Las Vegas, USA, as she had come to South Korea for a 3-month medical leave from her job.
Figure 4
|
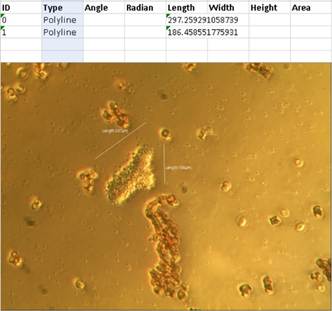
Figure 4 Stereomicroscopic features (pre-treatment) of a 61-year-old female patient who came from the U.S.A. The toxicology test revealed a small Graphene Oxide-like material (polyacrylamide hydrogel filaments or ribbons) / microchip (point 1), 297 micrometer dough-like inflammatory cells (point 3), mild inflammatory cells (point 2), and mild microrobots (point 2). There were no crenated red blood cells (RBCs) and no RBC rouleaux, resulting in a total score of 8. |
Figure 5
|
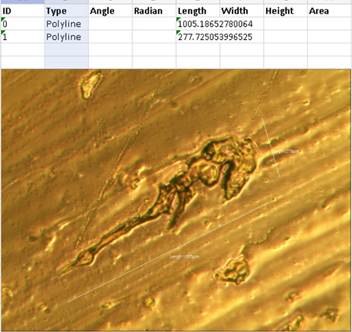
Figure 5 The stereomicroscopic features (pre-treatment) of a 61-year-old female patient who came from the U.S.A., revealed a metal-pin-like material measuring 1.005 micrometers. observed through the stereomicroscopy from her blood, which was extracted using the cupping method of Oriental medicine. |
Figure 6

|
Figure 6 The stereomicroscopic features (pre-reatment) of a 61-year-old female patient who came from
the U.S.A., revealed a 1,090 micrometers
of metal-tree root-like material and along with other golden colored substances with black-colored
meshy outer layers. These were observed in the stereomicroscopy from her
blood, which was extracted using the cupping method of Oriental medicine. The
substances resembled ribbons or rubbery-to-fibrous-looking clots containing
amyloid deposits that were obtained from blood vessels during the embalming
process. Grobbelaar et
al. (2021), Yuhong (2022) |
Figure 7
|
Figure 7 The stereomicroscopic features (Post-treatment) of a 61-year-old female patient who came from the U.S.A. Toxicology test revealed a 209-micrometer-sized Graphene Oxide-like material (polyacrylamide hydrogel filaments or ribbons) / microchip (point 3). Additionally, there were 114-micrometer dough-like inflammatory cells (point 2) with no inflammatory cells, no microrobots, mild crenated red blood cells (RBCs) (point 1), and no RBC rouleaux. The resultant total score is 7. |
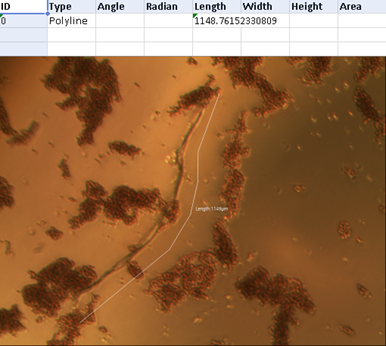
Patient 3: A 68-year-old male patient had not received a Covid-19 vaccination, nor had he undergone a PCR testing or confirmed SARS-CoV-2 infections; however, he likely experienced several unconfirmed SARS-CoV-2 infections. He presented strange headaches, nasal discharges accompanied by sudden coughing, chest tightness, intermittent dizziness, no tinnitus, but with mild tiredness and mild weaknesses. He also reported episodes of weak herpes simplex, lower back pain, coldness in the extremities. However, he had no limitations in motion, no depressive mood, no insomnia, but had a little decreased visual acuity, some brain fog, intermittent abdominal pain, indigestion, and some nausea. His blood chemistry tests prior to the treatment indicated hyperlipidemia (cholesterol 242 mg/dL, exceeding the normal range of 200 mg/dL, triglyceriede 312 > 150 mg/dL), pancreatitis (amylase 108 > 100 U/L), and myocarditis or myocardial ischemia (CK-MB 5.80 > 4.87 ng/mL). Before-treatment blood toxicology test yielded a total score of 22. Figure 8
His symptoms improved after the Cocktail medications and several days of intravenous Cocktail injections by the Cocktail protocol of the previous study.[3] His follow-up blood tests after the treatment revealed normal cholesterol levels (194 mg/dL), elevated triglycerides (206 mg/dL, with a normal range of <150 mg/dL), normal amylase (89 U/L, with a normal range of <100 U/L), and a normal cardiac enzyme level (CK-MB 2.05 ng/mL, with a normal range of < 4.87 ng/mL). Follow-up blood toxicology test indicated a total score of 3. Figure 9
Figure 8
|
Figure 8 The stereomicroscopic features (before treatment) of a 68-year-old male patient revealed a toxicology test that identified a large, elongated material resembling Graphene Oxide (polyacrylamide hydrogel filaments or ribbons) measuring 1,148 micormeters in length. This substance was found in the peripheral blood, resulting the total toxicology score of 22. |
Figure 9

|
Figure 9 The stereomicroscopic features observed post-treatment in a 68-year-old male patient indicated a toxicology test of the plasma revealed the presnece of Graphene Oxide-like material (polyacrylamide hydrogel filaments or ribbons) / microchip measuring a 289 micrometers in size (point 3). Additionally, there were no dough-like inflammatory cells, no inflammatory cells, no microrobots, no crenated red blood cells (RBCs), and no RBC rouleaux, resulting in a total score of 3. |
4. Discussion
Current terminology for long Covid is diverse; and it is called also as post-acute sequelae of Covid-19 infections (PASC), post-Covid-19 condition, post-Covid syndrome, and ongoing symptomatic Covid-19. Parums (2024) In an ICD-10 coding system, U09.9 denotes for long Covid patients with a heterogeneous array of symptoms, including fatigue, exertional dyspnea (breathing difficulty), decreased cognition, brain fog, coldness and numbness of the extremities, insomnia, joint pain, easy petechiae, and cardiac problems, all of which is represented in PASC. Pfaff et al. (2023) In the United States, the estimated number of long Covid was 37.8 millions in adults as of 2024, the percentage was 5.3% of adult population, and 21.5% of all women. Elflein (2024) Twenty-five symptoms reported by long Covid patients share similar clinical features with the 29 symptoms associated with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Wong and Weitzer (2021) It has been observed that long Covid patients are more likelyto be women, individuals from underprivileged and poor socioeconomic backgrounds rather than those in middle- or high-socioeconomic status, and unemployed rather than employed counterparts. Pfaff et al. (2023) Approximately 32.8% of hospitalized SARS-CoV-2 patients exhibited PASC and presented post-Covid conditions characterized by constitutional, respiratory, and nueropsychiatric symptoms. Nair et al. (2025) The risk of long Covid is potentially associated with Covid-19 vaccination and reinfections with different SARS-CoV-2 variants compared to the initial infection. Ballering et al. (2022) Chronic fatigue symptoms in long Covid patients have shown improvemtnts with low-dose naltrexone (LDN) and NAD (nicotinamide adenine dinucleotide)+ supplementation. Isman et al. (2024) Repurposed medications such as Methylphenidate, Duloxetine, and Brexpiprazole have been reported to alleviate self-reported fatigue, pain severity, tiredness upon awakening, and muscle stiffness. Manu (2022) However, a population-based nested case-control study indicated that inadequately treated PASC people had persistent symptoms even in the second year of long Covid. Peter et al. (2025)
Through the Yale RECOVERY and Yale LISTEN studies, Akiko Iwasaki proposed that long Covid was an “umbrella term” and provided four hypotheses for the possible mechanisms for the underlying cause of long Covid. Wilson (2024). First, persistent viral RNA or viral antigens have been detected in the blood, indicating an inadequate immune system reponse to eliminate them and resulting in an ongoing bodily injury. Second, there is evidence that Covid-19 can reactivate certain viruses such as herpesviruses or Epstein-Barr virus, potentially due to Covid-19 cause malfunctions in the body’s immune system. Third, Covid-19 may trigger dormant autoimmune disease to reactivate and to produce autoantibodies that cause inflammatory processes and tissue damage. Fourth, segments of the SARS-CoV-2 virus or viral RNA can prompt immune cells to release inflammatory cytokines, initiating tissue injury and triggering inflammatory cascades and chronic inflammations. If we accept that persistent viral RNA or viral antigens, or viral segments in the blood can contribute to long Covid, it follows that Covid-19 vaccinations can also cause long Covid because the Yale LISTEN study was reported that the individuals in the long Covid cohort exhibited free spike proteins for over 709 days following their Covid-19 vaccinations and the cohort had reduced both Th1 and Th2 CD4+ T helper cells. Bhattacharjee et al. (2025) The National Academies of Sciences, Engineering, and Medicine (NASEM) meeting for long Covid sought avoid using the term of “syndrome” because the word “syndrome” may dilute of having a physical basis or of formal ailments associated with the condition of the long Covid. Ely et al. (2024) However, this report proposes the inclusion of the term “syndrome” to long Covid for the clarification. By adding “syndrome” in the long Covid, the “long Covid syndrome” contains physical basis or formal ailment of Covid-19 vaccination sequelae, in addition to the definition of long Covid which was defined and established by NASEM meeting. When we say Covid-19 vaccination sequelae, we do not require proof of Covid-19 vaccination because non-vaccinated people who have been experiencing shedding phenomena also have similar toxic materials or toxicity scores as vaccinated people have as seen in this report. Table 3 shows that non-vaccinated people showed similar toxicity scores as those of vaccinated people both the pre-treatment period (15.70 ± 6.39 vs 11.89 ± 4.36) and the post-treatment period. (7.70 ± 3.20 vs 8.00 ± 3.20). VAIDS (vaccine-Acquired Immunodeficiency Syndrome) and VITT (vaccine-induced Immune Thrombotic Thrombocytopenia) represented that Covid-19 vaccinated people had lower immunity than that before the vaccination. Yamamoto (2022) Results of Table 3 satisfies or signifies two arguments. First, the toxicity (toxic material) scores along with symptoms and blood chemistry tests can help medical professionals to identify patients with the long Covid syndrome and evaluate their grade of severity of the long Covid syndrome. Second, the Cocktail medication (Covi Wonder) and the healing protocol worked significantly and effectively to relieve the symptoms of the patients with the long Covid syndrome and to alleviate toxicity in the blood of long Covid syndrome patients. However, there were some people, who were allergic to some of Cocktail medications, and who did not take those allergic medications but improved their conditions. Thus we may think that not all the medications of Cocktail treatment are necessary for the cure and to alleviate long Covid syndrome.
There are reports that there are environmental pollutions and sheddings from vaccinated people, that some components of Covid-19 vaccines are living things, and that Covid-19 vaccines have self-replicating and self-assembling nanoparticles. Lee and Broudy (2024), Jeon (2022) Accordingly, the duration of treatment or healing process cannot be limited to as 5 or 10 months but needs to be continued as long as environmental pollutions or sheddings continue. Since taking Cocktail medications for more than a year is a nuisance, some simplified method or form of Cocktail medications (Covi Wonder) is necessary and further study is warranted to make a simplified or easy way to take Cocktail medications for the healing of long Covid syndrome.
CDC estimated 5000 people died from long Covid, and if we add deaths induced by sequelae of Covid-19 injectables, which had 28 times higher general psychiatric adverse reactions than those of all other vaccines summed-up except Covid-19 vaccines Centers for Disease Control and Prevention. (2025), Thorp et al. (2025), the estimated death of long Covid syndrome will be much higher than that of long Covid which does not include any sequelae cases induced by Covid-19 injectables. Since many researchers inluding Ana M. Mihalcea showed toxic materials in the bloods in all the people they observed regardless of Covid-19 vaccinations or of SARS-CoV-2 infections, all of us may need a healing or treatments from a long Covid syndrome wherther we have symptoms or not. Mihalcea (2024)
In conclusion, the results indicate that the toxicity (toxic material content or toxicity severity) score and Cocktail treatments can help to diagnose and to alleviate the worldwide burdens of both the long Covid and the sequelae of Covid-19 vaccination.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
In this report, I want to honor Dr. Reiner Fuellmich, who pioneered civil rights movements against the so-called deep state program of SARS-CoV-2 and Covid-19 injectables (vaccines), but was sentenced to be in jail for 3 years and 9 months by the German judicial system which tried to muzzle the right opinions of the citizens.
REFERENCES
Ballering, A. V., van Zon, S. K. R., et al. (2022). Persistence of Somatic Symptoms After COVID-19 in The Netherlands: An Observational Cohort Study. The Lancet, 400(10350), 452–461. https://doi.org/10.1016/S0140-6736(22)01214-4
Bhattacharjee, B., et al. (2025). Immunological and Antigenic Signatures Associated with Chronic Illnesses After COVID-19 Vaccination. MedRxiv. https://doi.org/10.1101/2025.02.18.25322379
Centers for Disease Control and Prevention. (2025). Clinical overview of Long COVID. COVID-19 | CDC.
Elflein, J. (2024). Long COVID in the U.S.—Statistics & facts. Statista. Retrieved April 30, 2025,
Ely, E. W., Brown, L. M., & Fineberg, H. V. (2024). Long COVID Defined. The New England Journal of Medicine, 391, 1746–1753. https://doi.org/10.1056/NEJMsb2408466
Grobbelaar, L. M., Venter, C., Vlok, M., Ngoepe, M., Laubscher, G. J., Lourens, P. J., Steenkamp, J., Kell, D. B., & Pretorius, E. (2021). SARS-CoV-2 Spike Protein S1 Induces Fibrin(ogen) Resistant to Fibrinolysis: Implications for Microclot Formation in COVID-19. Bioscience Reports, 41(8), BSR20210611. https://doi.org/10.1042/BSR20210611
Hadanny, A., Zilberman-Itskovich, S., Catalogna, M., et al. (2024). Long-Term Outcomes of Hyperbaric Oxygen Therapy in Post-COVID Condition: Longitudinal Follow-Up of a Randomized Controlled Trial. Scientific Reports, 14, 3604. https://doi.org/10.1038/s41598-024-53091-3
Isman, A., Nyquist, A., Strecker, B., Harinath, G., Lee, V., Zhang, X., & Zalzala, S. (2024). Low-dose Naltrexone and NAD+ for the Treatment of Patients with Persistent Fatigue Symptoms After COVID-19. Brain, Behavior, & Immunity - Health, 36, 100733. https://doi.org/10.1016/j.bbih.2024.100733
Jeon, K-Y. (2024). Healing Protocols and Toxicology Tests for Sequelae of COVID-19 Injectables. Granthaalayah.
Jeon, K. Y. (2022). Moving and Living Micro-Organisms in the COVID-19 Vaccines - Prevention, Early Treatment Cocktails for COVID-19, and Detoxification Methods to Reduce Sequelae of COVID-19 vaccines. American Journal of Epidemiology and Public Health, 6(1), 001–006. https://doi.org/10.37871/ajeph.id50
Lee, Y. M., & Broudy, D. (2024). Real-Time Self-Assembly of Stereomicroscopically Visible Artificial Constructions in Incubated Specimens of mRNA Products Mainly from Pfizer and Moderna: A Comprehensive Longitudinal Study. International Journal of Vaccine Theory, Practice, and Research, 3(2). https://doi.org/10.56098/586k0043
Manu, P. (2022). Repurposing Drugs for Post–COVID-19 Fatigue Syndrome: Methylphenidate, Duloxetine, and Brexpiprazole. American Journal of Therapeutics, 29(2), e229–e230. https://doi.org/10.1097/MJT.0000000000001471
Mihalcea, A. M. (2024). TransHuman: Overcoming the Global Depopulation Agenda - Volume II: Self-Assembling Nanotechnology in Medications, Geoengineering Effects, and Mesogen Microchips – Treatments and Antidotes.
Nair, C. V., Krishnakumar, M., Gutjahr, G., et al. (2025). Early biomarkers in Hospitalized Patients as Predictors of Post-Acute Sequelae of SARS-CoV-2 Infection: A One-Year Cohort Study. BMC Infectious Diseases, 25, 398. https://doi.org/10.1186/s12879-025-10619-w
Parums, D. V. (2024). Long COVID or Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) and the Urgent Need to Identify Diagnostic Biomarkers and Risk Factors. Medical Science Monitor, 30, e946512. https://doi.org/10.12659/MSM.946512
Peter, R. S., Nieters, A., Göpel, S., Merle, U., Steinacker, J. M., Deibert, P., et al. (2025). Persistent Symptoms and Clinical Findings in Adults with Post-Acute Sequelae of COVID-19/post-COVID-19 Syndrome in the Second Year After Acute Infection: A Population-Based, Nested Case-Control Study. PLoS Medicine, 22(1), e1004511. https://doi.org/10.1371/journal.pmed.100451
Pfaff, E. R., Madlock-Brown, C., Baratta, J. M., et al. (2023). Coding long COVID: Characterizing a New Disease Through an ICD-10 lens. BMC Medicine, 21, 58. https://doi.org/10.1186/s12916-023-02737-6
Thorp, J., Rogers, C., Cosgrove, K., Hatfill, S., Breggin, P., Pinsky, D., & McCullough, P. (2025). Association between COVID-19 Vaccination and Neuropsychiatric Conditions. Preprints. https://doi.org/10.20944/preprints202504.1099.v1
Wilson, E. M. (2024). The long COVID Puzzle: Autoimmunity, Inflammation, and Other Possible Causes. Yale Medicine. Retrieved April 30, 2025.
Wong, T. L., & Weitzer, D. J. (2021). Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)-A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina (Kaunas), 57(5), 418. https://doi.org/10.3390/medicina57050418
Yamamoto, K. (2022). Adverse Effects of COVID-19 Vaccines and Measures to Prevent Them. Virology Journal, 19(1), 100. https://doi.org/10.1186/s12985-022-01831-0
Yuhong, D. (2022). Why Strange Clots form After mRNA Jabs, Treatments to Consider. The Epoch Times.
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2025. All Rights Reserved.

