
Homoeopathic Management of Chronic Pediatric Idiopathic Thrombocytopenic Purpura: Case series
Kundu Tapas 1 ![]()
![]() ,
Kumat Omkar 2
,
Kumat Omkar 2![]()
![]() , Mirza Gulfisha 3
, Mirza Gulfisha 3![]() , Kundu Rita 4
, Kundu Rita 4![]() , Singh Trupti 3
, Singh Trupti 3![]()
1 Principal Investigator - Homoeopathy in
Haemophilia, C/O Sakha the Centre of Research and Charity,
Upnagar, Professor and HOD of Medicine, Motiwala
(National) Homoeopathic Medical College, Nashik, Maharashtra, India
2 Co-Investigator, Homoeopathy in Haemophilia, C/O Sakha the Centre of Research and Charity, Upnagar, Nashik, Maharashtra, India
3 Research Associate, Homoeopathy in Haemophilia, C/O Sakha the Centre of Research and Charity, Upnagar, Nashik, Maharashtra, India
4 Professor and HOD of Physiology, Motiwala (National) Homoeopathic Medical College, Nashik, Maharashtra, India
|
|
|
ABSTRACT |
|
|
Idiopathic Thrombocytopenic purpura (ITP) is an autoimmune disorder characterized by decrease in platelets count in blood, leading to manifestations like spontaneous bleeding such as epistaxis, petechiae, ecchymotic patches or painful bruises, gum bleeding or fatal haemorrhages. Here we present three cases of ITP, its manifestation and homoeopathic management. Wong Baker pain rating scale, Adaptive and Maladaptive behavioral scale were used for assessment. A Naranjo criterion for homoeopathy, casual attribution (MONARCH) inventory was used to assess individual curative response of each case, which elucidated the role of homoeopathy in management of ITP. Homeopathic medicine effectively managed the episodes of bleeding and other symptoms in case of chronic pediatric Idiopathic Thrombocytopenic purpura (ITP). |
|||
|
Received 28 October 2022 Accepted 29 November 2022 Published 09 December 2022 Corresponding Author Kumat Omkar, dromkarkumat@gmail.com
DOI10.29121/granthaalayah.v10.i11.2022.4898 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2022 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: ITP, Hematological Cases, Bleeding,
Homoeopathy, Autoimmune, Case Series |
|||
1. INTRODUCTION
Idiopathic Thrombocytopenic purpura (ITP) is an autoimmune
blood disorder characterized by decrease in platelets count in blood. The
normal range of platelets in healthy human being is from 150,000 to 450,000/cu
mm1. The word Idiopathic refers to unknown cause, thrombocytopenia
means decrease in platelets, and purpura refers to purple discoloration of the
skin as bruise. ITP no longer considered as idiopathic, now known as Immune
Thrombocytopenic Purpura. McCRAE KE. (2011)
It only has antibodies against platelets; therefore it
is isolated thrombocytopenia. The Auto antibodies are formed against GP IIb/
IIIa. These antibodies get attached to GP IIB/IIIa which are engulfed by
macrophages and further destroyed in spleen causes extra vascular destruction.
Generally, platelet count >50,000 without bleeding or symptoms are not given
treatment, but platelets count <20,000- 50,000 with bleeding are considered severe which causes spontaneous bleeding Ghulam (2020) such as
epistaxis, petechiae, ecchymotic patches or painful
bruises, gum bleeding. There are two forms of ITP.1) Acute Thrombocytopenic
purpura: Usually affects young children ages between 2 to 6 yrs. It is observed
most of those children are previously diagnosed or affected by viral infection.
The acute usually starts suddenly and it is self-limiting with the recovery
rate in 50%- 70% of patients. Mushtaq et al. (2014)
2) Chronic Thrombocytopenic purpura: the onset happen
at any age, symptoms last a min, 06 months, several years or lifetime. Idiopathic Thrombocytopenic
Purpura [2022]
ITP patient suffers from bruising pain, petechial patches, nose, gum
bleeding. Subarachnoid, intra cerebral haemorrhage or other internal bleeding
are very serious possible complications of ITP. In women’s heavy menstrual
bleeding is seen, blood in urine and stools. Low Platelets Count Idiopathic
Thrombocytopenia Purpura (ITP) (2011)
The majority of children require no treatment and in 80–85% of cases the
disorder resolves within 6 months. About 15–20% of children develop a chronic
form of ITP, which, in some cases, resembles the more typical adult disease.
Chronic ITP in childhood has an estimated incidence of 0.46 per 100 000
children per year Reid (1995) and prevalence
of 4.6 per 100 000 children at any one time ITP
(2003). The complications of
chronic ITP can be fatal. Management is predicted primarily on the severity of
thrombocytopenia and bleeding. Pediatric patients with ITP from infancy to adolescence
exhibit heterogeneity in clinical, demographic, and treatment factors.
2. CASE REPORTS
2.1. Case 1
On 1/04/2017; A 08-year-old boy presented in the OPD with complaints of recurrent epistaxis since 3 ½ years. K/C/O ITP.
2.1.1. Past history
The bleeding frequency is around 7-8 episodes of epistaxis every month which accounts for an average of more than 300 episodes till now. The duration of bleeding last for 02 hrs. The onset was usually sudden, mostly aggravated during daytime. Bruised blue, purple rashes on and off at random sites. Usually managed acutely with standard management according to severity of the episode.
2.1.2. Laboratory findings
Table 1
|
Table 1 |
|||||
|
Date |
24/02/2017 |
25/02/2017 |
27/02/2017 |
1/03/1017 |
24/03/2017 |
|
Hb |
11.8 |
11.0 |
11.6 |
|
10.2 |
|
Platelets |
56000 |
60,000 |
1,20000 |
<20,000 |
71,000 |
Family history- there is no family history of any bleeding or genetic disorders. The marriage between parents is non-consanguineous.
Mind symptom- very diligent about his work and cowardice in nature.
Physical generals-thirstless, very marked desire for sweets and aversion for vegetables
2.1.3. Assessment with scales
1) Pain score during bleed 8.
2) Adaptive and Maladaptive Behavior scales-
Activity level: Very active- score-6
Cooperation: Cooperative- score-6
Communication skills: shy but warms up quickly- score-4
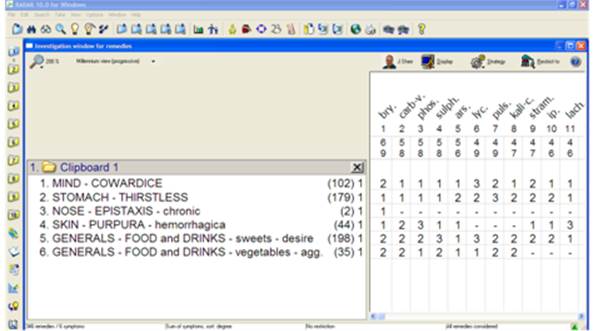
Repertorization and remedial analysis-
· MIND –COWARDICE
· STOMACH –THIRSTLESS
· NOSE-EPISTAXIS – chronic
· SKIN -PURPURA – hemorrhagica
· GENERALS-FOOD and DRINKS-sweets –desire
· GENERALS - FOOD and DRINKS - vegetables - agg.
Figure 1
|
Figure 1 |
2.1.4. Remedy
1) Bryonia Alba 30 CH / 3 Doses in Sugar of Milk Powder / 24 hourly.
2) Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month.
Table 2
|
Table 2 Follow Up Chart-Case 1 |
|||
|
Date of visit/follow up |
Symptomatology |
Treatment |
Justification |
|
2/05/2017 |
- Bleeding episode frequency came down from 7-8 times per month to 3-4 times per month. -The duration of bleeding reduced from 2 hours to around 20 minutes. -Platelet count -55,000 -Petechial haemorrhage frequency also reduced. |
Bryonia Alba 30 CH / 1 Dose in Sugar of Milk Powder / Stat. Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
The patient was better. |
|
2/8/2017 |
-Two episodes of epistaxis. With reduced severity and duration to 10 minutes. -No petechial haemorrhages seen |
Bryonia Alba 30 CH / 1 Dose in Sugar of Milk Powder / Stat. Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
The patient was better. |
|
2/3/2019 |
-Epistaxis 1 day ago, which lasted for 10 minutes, with mild pain and severity. -No petechial haemorrhages seen |
Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
The patient was better. |
|
5/1/2022 |
-No episode of epistaxis since last 3 years |
Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
The patient had no complaints. |
Table 3
|
Table 3 Assessment of Scale-Case 1 |
|||
|
|
Scale Used |
Before |
After |
|
1 |
Adaptive /maladaptive (modified)
behavioural scale- |
|
|
|
|
Activity level- score |
6 |
6 |
|
|
Co-operation- score |
6 |
8 |
|
|
Communication Skill- score |
4 |
6 |
|
2 |
Wong baker pain rating scale |
8 |
0 |
2.2. Case 02
27/12/2019; A 07-month age, male child was brought to OPD, with presenting complaints of eruption over body due to allergic reaction of allopathic medicine. He had K/C/O ITP and Steve Johnson Syndrome.
2.2.1. Past history
of fever. He had habit of bed wetting, sensitive to allopathic medicine.
2.2.2. Laboratory findings
Bone marrow aspiration reports mentioned clinical
impression of ITP. CBC reports: HB-9.5%, PLT:-12x103,
WBC: 6.8x103, RBC:4.02 x 106.
Mind symptoms –contradictive and very stubborn.
Physical generals-desires spicy.
2.2.3. Assessment with scales
1) Pain score during bleed 6.
2) Adaptive and Maladaptive Behavior scales-
Activity level: Very active- score-6
Cooperation: Cooperative- score-6
Communication skills: shy but warms up quickly- score-6
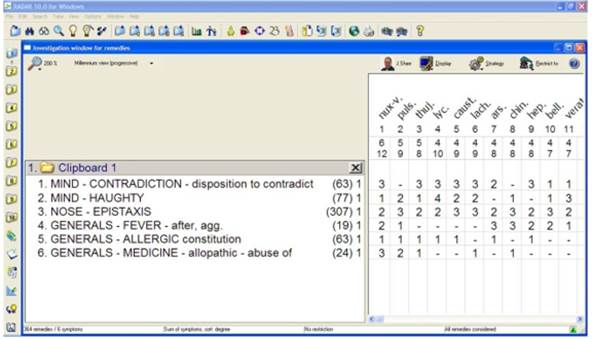
2.2.4. Repertorization and remedial analysis
·
MIND -CONTRADICTION-disposition to contradict
·
MIND –HAUGHT
·
NOSE –EPISTAXIS
·
GENERALS-FEVER-after, agg.
·
GENERALS-ALLERGIC constitution
·
GENERALS
- MEDICINE - allopathic - abuse of
Figure 2
|
Figure 2 |
2.2.5. Remedy
Considering the nature and totality of symptoms he was prescribed -
1) Nux Vomica 200 CH / 3 Doses in Sugar of Milk Powder / 1 Dose stat then SOS.
2) Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month.
Table 4
|
Table 4 Follow Up Chart –Case 2 |
|||
|
Date of visit/follow up |
Symptomatology |
Treatment |
Justification |
|
27/12/2019 |
Allergic reaction better. No bleeding episode. |
Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
The patient was better. |
|
29/1/2020 |
Epistaxis with cold coryza and fever. |
Lachesis Muta 200 CH /1 dose in Sugar of Milk Powder / Stat. Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
Indication through Repertory and HMM. |
|
2/03/2020 |
Patient was better with no fresh complains. |
Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
The patient was better. |
Table 5
|
Table 5 Assessment of Scale –Case 2 |
|||
|
|
Scale
Used |
|
|
|
|
|
Before |
After |
|
1 |
Adaptive / maladaptive (modified) behavioural scale- |
|
|
|
|
Activity level- score |
6 |
6 |
|
|
Co-operation- score |
6 |
8 |
|
|
Communication Skill- score |
6 |
6 |
|
2 |
Wong baker pain rating scale |
6 |
0 |
2.3. Case no. 03
On 5/1/21; A 07-year-old boy known case of ITP came with complaints of epistaxis since 03 years < night. Bilateral profound sensory neural hearing loss. Skin itching with purplish discoloration.
2.3.1. Past history
Dengue fever twice at age of 02 years and 5 years.
2.3.2. Family history
Parents had consanguineous marriage.
2.3.3. Laboratory findings
Blood reports Hb-9.9%, RBC: 3.58, WBC: -4800, Plt: 1.10.
2.3.4. Mind symptom
Fear of cats, dogs. unable to concentrate.
2.3.5. Physical generals
Anemia, sleeps on abdomen.
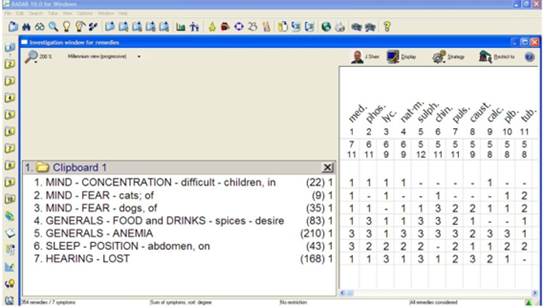
2.3.6. Repertorization and remedial analysis
·
MIND - CONCENTRATION - difficult -
children, in
·
MIND -
FEAR - cats; of
·
MIND - FEAR - dogs, of
·
GENERALS - FOOD and DRINKS -
spices – desire
·
GENERALS – ANEMIA
·
SLEEP - POSITION - abdomen, on
·
HEARING – LOST
Figure 3
|
Figure 3 |
2.3.7. Remedy
By taking totality of symptoms, he was prescribed -
Medorrhinum 200 CH / 3 Doses in Sugar of Milk Powder / Weekly once.
Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month.
2.3.8. Assessment with scales
1) Pain score during bleed 8.
2) Adaptive and Maladaptive Behavior scales-
Activity level: Very active- score-6
Cooperation: Cooperative- score-4
Communication skills: shy but warms up quickly- score-4
2.3.9. Follow up
he had bleeding episode 3-4 times after which there was no episode, was prescribed – Medorrhinum 1M/ 1 dose - stat. There was itching which reduced day by day with no bleeding episode till now.
Table 6
|
Table 6 Follow Up Chart-Case 3 |
|||
|
Date of visit/follow up |
Symptomatology |
Treatment |
Justification |
|
18/2/2021 |
No bleeding episode. Itching persist. |
1) Medorrhinum 1 M/single dose in sacchrum lactis powder. 2) Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
Bleeding episodes were better, but medicine was repeated for the skin symptoms. |
|
3/5/2021 |
No bleeding episode. Itching reduced. |
Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
Patient was better. |
|
14/07/2021 |
No bleeding episode and patient was healthy in general. |
Rubrum 30 / 2 Drachm in globule no 30 / 4-0-4 globules / 1 Month. |
Patient was better |
Table 7
|
Table 7 Assessment of Scale-case 3 |
|||
|
|
Scale
Used |
|
|
|
|
|
Before |
After |
|
1 |
Adaptive /maladaptive (modified) behavioural scale- |
|
|
|
|
Activity level- score |
6 |
6 |
|
|
Co-operation- score |
4 |
8 |
|
|
Communication Skill- score |
4 |
6 |
|
2 |
Wong baker pain rating scale |
8 |
0 |
Table 8
|
Table 8 Patient Outcome Assessment on Modified Naranjo Criteria in Homeopathy (MONARCH) Assessment of Both Patient are Separated by a / (H-343/H-361) |
||||||||
|
Domains |
Yes |
No |
Not Sure or N/A |
|||||
|
|
Case 1 |
Case 2 |
Case 3 |
Case 1 |
Case 2 |
Case 3 |
|
|
|
1 |
Was there an improvement in the main symptom or condition for which the homeopathic medicine was prescribed? |
+2 |
+2 |
+2 |
|
|
- |
- |
|
2 |
Did the clinical improvement occur
within a plausible timeframe relative to the drug intake? |
+2 |
+1 |
+1 |
|
|
- |
- |
|
3 |
Was there an initial aggravation of symptoms? |
|
|
|
+1 |
+1 |
+1 |
- |
|
4 |
Did the effect encompass more than the main symptom or condition (i.e., were other symptoms ultimately improved or changed)? |
+1 |
+1 |
+1 |
|
|
- |
- |
|
5 |
Did overall well-being improve? (Suggest using validated scale) |
+1 |
+1 |
+1 |
|
|
- |
- |
|
6A |
Direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? |
0 |
0 |
0 |
|
|
- |
- |
|
6B |
Direction of cure: did at least two of the following aspects apply to the order of improvement of symptoms: –from organs of more importance to those of less importance? –from deeper to more superficial aspects of the individual? –from the top downwards? |
0 |
0 |
0 |
|
|
- |
- |
|
7 |
Did “old symptoms” (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? |
0 |
0 |
0 |
|
|
- |
- |
|
8 |
Are there alternate causes (other than the medicine) that—with a high probability—could have caused the improvement? (Consider known course of disease, other forms of treatment, and other clinically relevant interventions) |
+1 |
+1 |
+1 |
|
|
- |
- |
|
9 |
Was the health improvement confirmed by any objective evidence? (e.g., laboratory test, clinical observation, etc.) |
+2 |
+2 |
+2 |
|
|
- |
- |
|
10 |
Did repeat dosing, if conducted, create similar clinical improvement? |
+1 |
+1 |
+1 |
|
|
- |
- |
|
|
Total score |
11 |
10 |
10 |
|
|
|
|
|
Note: Maximum score=13, minimum score = -6 |
||||||||
3. DISCUSSION
Acute immune thrombocytopenic purpura (ITP) being autoimmune affects about 2–8 out of 100,000 children per year Blanchette and Carcao (2000), B. Bussel, (2001), C. Kuhne (2003). Acute and chronic idiopathic thrombocytopenic purpura (ITP) is traditionally based on the duration of thrombocytopenia at the cut-off point of 6 months after diagnosis Imbach et al. (2006). There are no randomized trials to support the effectiveness of any specific approach in treatment of ITP Vesely et al. (2003). This article presents 3 case reports of the diagnosed cases of ITP and its homoeopathic management. A Thorough case taking was done to obtain the individualistic features the case and important and characteristic points are presented. The medicine was prescribed using Schroyens F., Synthesis 9.0 repertory from RADAR 10.0 software sand differentiation from homoeopathic Materia Medica and considering the dominant miasm. All three cases were among the pediatric age group and were chronic in nature. The commonest form in pediatric age group is acute ITP, which resolves spontaneously within 6 months. But these three cases where chronic form of ITP which needed intervention. Amongst the three cases only one case revealed consanguinity of marriage between parents. This case was more genetically affected as it had profound sensory neural bilateral deafness, whereas other two cases had no such genetic disorder along. Two cases had past history of viral fevers. Epistaxis and skin symptoms were common presentation in all three cases. Wong Baker pain rating scale and adaptive /maladaptive behavioral scale were used for assessment. Modified Naranjo criteria for homoeopathy, casual attribution (MONARCH) inventory was used to assess individual curative response of each case, which elucidated the role of homoeopathy in management of ITP.
Individualised homoeopathic medicine Bryonia alba Figure 1, Nux Vomica Figure 2, and Medorrhinum Figure 3 were used respectively in three cases for treatment of ITP. The selection was based on homeopathic principles of similimum. The homoeopathic medicines improved condition of the patient both physically and mentally. Reporting of case is in accords to HOM-CASE-CARE guidelines Van Haselen (2016) . A case series of only 3 case is however inadequate to conclude the exact efficacy of homoeopathy in ITP, for which further control trials are necessary. Platelet counts did not increase significantly yet bleeding control was achieved with the medicines. Therefore, more elaborative diagnostic test is needed to know the exact mechanism of bleeding control.
4. Conclusion
Homoeopathic medicines managed effectively the cases of idiopathic thrombocyotopenic purpura.
5. Declaration of Patient Consent
The authors certify that they have obtained appropriate patient consent in written from the parents. The parents have given consent clinical information for the sake of scientific interest and publication of data.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
None.
REFERENCES
Bussel, J. B. (2001). Novel Approaches to Management of Immune Thrombocytopenic Purpura : Results of Recent Trials. ASH Meeting Orlando (FL) USA, Dec 7-11, 2001. Blood Education Program 2001, 5288- 5305.
Blanchette, V., And Carcao, M. (2000). Approach to the Investigation and Management of Immune Thrombocytopenic Purpura in Children. Semin Hematol. 37, 2991- 3006. https://doi.org/10.1016/S0037-1963(00)90108-2.
C. Kuhne T. (2003). Investigation And Management of Newly
Diagnosed Childhood Idiopathic Thrombocytopenic Purpura : Problems and Proposed
Solutions. Journal Pediatr Hematol Oncol 25, 524- 52. https://doi.org/10.1097/00043426-200312001-00006.
Chandran, R. (2019). Pain Assessment in Children Using a Modified Wong Baker Faces Pain Rating Scale. International Journal of Clinical Preventive Dentistry. 15(4), 202-5. https://doi.org/10.15236/ijcpd.2019.15.4.202.
Ghulam, Y. (2020). Cure of Immune Thrombocytopenic Purpura: A Homeopathic Approach. GSC Biological and Pharmaceutical Sciences. 10(3), 085-8. https://doi.org/10.30574/gscbps.2020.10.3.0053.
ITP A. (2003). Guidelines for the Investigation and Management
of Idiopathic Thrombocytopenic Purpura in Adults, Children and in Pregnancy. Br
J Haematol. 120(1), 574-96.
https://doi.org/10.1046/j.1365-2141.2003.04131.x.
Idiopathic Thrombocytopenic Purpura [Internet]. Google.Com. [2022].
Imbach, P., Kühne, T., Müller, D., Berchtold, W., Zimmerman, S., Elalfy, M., and Buchanan, G.R. (2006). Childhood ITP : 12 Months Follow-Up Data from the Prospective Registry I of The Intercontinental Childhood ITP Study Group (ICIS). Pediatric Blood and Cancer. 46(3), 351-6. https://doi.org/10.1002/pbc.20453.
Lamba, C.D., Gupta, V.K., Van Haselen R, Rutten, L., Mahajan, N., Molla, A.M., and Singhal, R. (2020). Evaluation of the Modified Naranjo Criteria for Assessing Causal Attribution of Clinical Outcome to Homeopathic Intervention as Presented in Case Reports. Homeopathy, 109(04), 191-7. https://doi.org/10.1055/s-0040-1701251.
Low Platelets Count Idiopathic Thrombocytopenia Purpura (ITP) (2011). Homoeopathy Treatment and Homoeopath.
McCRAE
KE. (2011). Immune Thrombocytopenia: No Longer 'Idiopathic'. Cleveland
Clinic Journal of Medicine. 78(6), 358. https://doi.org/10.3949/ccjm.78gr.10005.
Mcgrew, K.S., and Bruininks, R.H. (1990).Defining Adaptive and Maladaptive Behavior Within a Model of Personal Competence. School Psychology Review. 19(1), 53-73. https://doi.org/10.1080/02796015.1990.12087338.
Mushtaq, N., Alam, M.A., and Fadoo, Z. (2014). Idiopathic Thrombocytopenic Purpura in Children : A 10 Years' Experience at Tertiary Care Hospital. J Pak Med Assoc. 64(12), 1358-62.
Van Haselen, R.A. (2016). Homeopathic Clinical Case Reports :
Development of a Supplement (HOM-CASE) to the CARE Clinical Case Reporting
Guideline. Complementary Therapies In Medicine, 25, 78-85. https://doi.org/10.1016/j.ctim.2015.12.019.
Vesely, S.K., Perdue, J.J., Rizvi, M.A., Terrell,
D.R., And George, J.N. (2003). Management of Adult Patients With
Persistent Idiopathic Thrombocytopenic Purpura Following Splenectomy. Annals of
Internal Medicine, 140, 112-120. https://doi.org/10.7326/0003-4819-140-3-200402030-00012.
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2022. All Rights Reserved.

