
Fire Safety Compliance among Hospital Buildings: A Case Study from Nepal-Asia
Chandramani Bashyal 1
![]() , A.K. Mishra 2
, A.K. Mishra 2![]()
![]() , P.S. Aithal 3
, P.S. Aithal 3![]()
![]()
1 Master's Scholar United Technical
College, Affiliated to Pokhara University, Bharatpur
Metropolitan, Nepal
2 Associate Professor, United Technical
College, Affiliated to Pokhara University, Bharatpur
Metropolitan, Nepal
3 Professor
and Vice-Chancellor, Srinivas University, Mangalore, India
|
|
|
ABSTRACT |
|
|
Purpose: Hospital building is more sensitive to fire as it has large number of patients who might need assistance during evacuation. The assessment focuses to the Compliance for fire safety by accessing different standards; availability of equipment and systems, exit requirements and awareness among the departmental staffs of Hospitals. Design/Methodology/Approach: The study confined to the 4 hospitals from Bharatpur Metropolitan, Nepal based on judgmental sampling viz; Bharatpur Hospital, BP Koirala Memorial Cancer Hospital, College of Medical Science and Chitwan Medical College building. Literature review was done followed by observation with checklist, questionnaire survey and key informant interview. Findings/Result: The study revealed that the fire safety preparedness was not a priority in the hospitals. All hospital buildings were designed following National building codes. Both private and public Hospitals, practically every one of them uncover a similar degree of readiness. Bharatpur hospital lacked many firefighting equipment such as smoke detector, heat detector, fire alarm and water hose reel. Water sprinkle was missed on all hospitals. Obstruction was found in the escape route. Lacked exit signs and floor indications. Staffs were found aware about the general component of the structure like structure plan, area for exit and assembly points but lacked awareness on emergency procedure. Originality/Value: This
research complements the existing building code requirements and fire safety
implementation especially for hospital building as Nepal is not having
specific provisions for hospitals fire safety. It is assumed to be applicable
for policy making in concerned authority & forms basis for further
research. |
|||
|
Received 15 August 2022 Accepted 15 September 2022 Published 31 October 2022 Corresponding Author A.K.
Mishra, anjaymishra2000@gmail.com
DOI10.29121/granthaalayah.v10.i10.2022.4827 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2022 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Fire Safety Provisions, Firefighting
Equipment Availability, Standard of Fire Safety, Exit Requirements, Aware |
|||
1. INTRODUCTION
Fire hazard is the most common hazard, which is present in all areas of life. A fire can take dozens of lives and destroy hundreds of livelihoods in a minute. Nepal’s largest fire occurred at Singha Durbar in 1971, the Bhirkuti paper factory in 1984, and the Bhutanese camps of Jhapa in 2011. Nepal pay’s a heavy price in lives and properties due to fire Mishra and Shrestha (2017), Mishra and Aithal (2022), Lama and Mishra (2022).
Fire safety is important in any building but in hospitals
there are many patients who are either too injured, sick, unconscious and some
patients are receiving vital treatments or connected to machines. Moving these
people is slower and often very difficult.
At first Fire safety was assured through code here in 1994 A.D. Later
NBC 206, Architectural Design Requirements has been introduced in 2015 AD UNDP
(2009), Mishra and Aithal
(2021)
Hospital/ clinic Fire can have grave ramifications for patients, wellbeing staff and its foundation. One of the essential goals of fire wellbeing is to securely ensure the clearing of the multitude of inhabitants from a structure. Particularly in medical services offices for example Clinic the departure strategies are more mind boggling than in a normal structure. This is because of different reasons, for example, the enormous number of patients expecting help to empty, or the time expected to plan patients expecting help to clear or the time expected to plan patients for helped departure. Patients ought to at first be moved from areas of chance to safe regions.
The essential point of a clinic office is to not empty patients except if totally important. Thus, unique consideration ought to be centered on appropriate anticipations and concealment methods to stay away from this worst situation imaginable. Full clearing of a clinic ought to for the most part be considered if all else fail when moderation or other crisis reaction endeavours are not supposed to keep a protected consideration climate. Concealment gear should be promptly open to battle these flames. Staff individuals from the wellbeing office need to know about how to utilize the hardware and to stay away from alarm. Independence at the unit level is significant in light of the fact that convenient correspondence from emergency clinic pioneers might be troublesome or even unimaginable; worker at each level should know quickly what to do in their space WHO (2014).
In Nepal few research has been done about fire safety management and rarely at hospital buildings. This study was present the fire safety preparedness at the Bharatpur Hospital, BPKMC Hospital, CMS, and CMC buildings of Bharatpur Metropolitan city.
Fire safety standard code of NBC 107, 1994 seems insufficient for addressing the minimum standards of fire safety preparedness among commercial building of Kathmandu valley due to lack of clear provision and institutional provision for its implementation. This research will complement the existing building code requirements and fire safety implementation.
2. STATEMENT OF PROBLEMS
Nepal is vulnerable to a variety of hazards; fire is one of the major. Fire is a danger which can cause damages to life, liberty, and property if it caught in residential area, however the occupancy of hospital are not only capable doctors, nurses, and staff but also patients who might not be in a position to cope with the fire. So, hospital building must be prepared to cope in an emergency situation with fire to reduce the impact preparedness might be ensure in context of Bharatpur Metropolitan city. Rarely any study in this area has been conduct yet, so the researcher is keen to conduct the research in the area as Fire safety preparedness is an indispensable procedure that must be learnt by all staffs Barile et al. (2018), Irene et al. (2009). Fire safety preparedness in the study has been operationally defined in the term of availability of firefighting equipment and system, exit requirement and awareness of staff only.
It is an attempt to complement the techno-legal documents such as National Building Code and by laws for assuring fire safety preparedness among hospital building through the standard improvisations by drawing the attention of policy member, practitioner architecture and engineers and authority of concern hospital to improve their hospital's safety against fire. The study also highlights the requirements of the equipment and systems along with awareness among the concerned for fire safety preparedness.
3. OBJECTIVES
To access the evacuation and preparedness plan in terms of exit requirements, availability of firefighting equipment and fire protection systems along with awareness of fire fighting among the staffs at the selected hospital buildings in Bharatpur Metropolitan city.
4. LITERATURE REVIEW
4.1. COMPARISON OF DIFFERENT STANDARDS IN TERMS OF EXIT REQUIREMENTS
NBC107:1994 was contrasted and IS 1644: 1988, Code of training for fire wellbeing in structures and OSHA (USA) standard to feature the benefits and weaknesses of the NBC107:1994. Codes have been analysed as given in plain structure.
4.1.1. COMPARISON
OF EXIT ROUTE REQUIREMENTS
Table 1
|
Table 1 Exit Route |
||
|
NBC
107: 1994 |
IS
1644:1988 |
OSHA standard, USA |
|
clearing
at brief time frame |
Enclosed
type |
Route
must be permanent |
|
free
of any obstructions and no resistance to movement |
One
exit directly opens to street |
Arrangement
for quick escape |
|
clearly
visible |
Door
locks prohibited |
Unobstructed |
|
preferably
with proper signs |
Mirror
not allowed |
Alternate
route far from each-other |
|
Continuous
and not interrupt into private space. |
||
The Table 1 shows that the NBC 107: 1994 has referenced that exit will meet the base prerequisite of time and be liberated from check. IS 1644:1988 has referenced that, encased exit will be given, and mirror will be stayed away from. Exit will expect to be nonstop however where it will lead was not referenced. If there should be an occurrence of Hong Kong Standard obviously exit will straightforwardly prompt extremely spot of wellbeing. Whereas OSHA has mentioned the route must be permanent and there should be an alternate route far from each-other.
4.1.2. COMPARISON OF STAIRCASE REQUIREMENT
Table 2
|
Table 2 Staircase Requirement |
||
|
NBC:107 |
IS
1644:1988 |
OSHA standard,
USA |
|
Min
Width 1.5 m |
No
living space or store open into stairs |
stairs
that continue beyond the level on which the exit discharge is located must be
interrupted at that level by doors, partitions, or other effective means |
|
Exit
door of staircase at ground, open at ultimate place of safety |
clearly
indicate the direction of travel leading to the exit discharge |
|
|
beam/column
and other shall not reduce the headroom and width of stair |
Separate
stair for occupants & fire service personnel. |
|
|
>500m2
on each floor area =nos. of stair 2 |
>500m2
on each floor area and above 15 m height min 2 stairs |
|
In NBC 107: 1994 just number of flight of stairs and width of the flight of stairs was referenced. Detail like clear headroom of flight of stairs was not notice which was given in IS 1644:1988. No position and game plan of flight of stairs has been made. IS 1644:1988 has additionally referenced that living space will not open in flight of stairs. Hong Kong Standard has referenced that no leave entryway while swing diminish the compelling width of landing. While OSHA has referenced the level past the leave release should be interfered with at that level by entryways, parcels, or other viable means and there should be a different step for tenants and fire administration staff.
4.1.3. COMPARISON OF PRESSURIZATION OF STAIRCASE
Table 3
|
Table 3 Pressurization of Staircase |
||
|
NBC
107: 1994 |
IS 1644:1988 |
OSHA standard, USA |
|
Rise
the pressure slightly above the adjacent side of building to prevent ingress
of smoke in escape rout |
Occupant
load for each floor must not decrease in the direction of exit discharge. |
|
|
Must
have adequate lighting |
||
|
Vertical ventilation for heat
and smoke |
||
|
Same
number of stairs for each partition |
||
Compression of flight of stairs was not referenced in
NBC:107 1994. It was remembered for IS 1644: 1988. OSHA has referenced the
tenant limit should not diminish in that frame of mind of leave release and
have vertical ventilation for intensity and smoke. Compression of flight of
stairs assists with forestalling smoke passage to safeguarded get away from
course and improve perceivability.
4.1.4. COMPARISON OF EXIT ROUTE AND TRAVEL DISTANCE REQUIREMENTS
Table 4
|
Table 4 Exit Route and Travel Distance Requirements |
||
|
NBC
107: 1994 |
IS
1644:1988 |
OSHA standard,
USA |
|
Max 20
m |
Max
30m |
Exit
route must be reasonably straight and have smooth, solid, substantially level
walkway |
|
Min 15
m at dead end |
Max 100
feet |
|
Head out distance to the exit was under 20 m by NBC 107 and max 30 m by IS 1644:1988, which was restricted to 20 m however travel distance from impasse. Hong Kong referenced max 30m. while OSHA has referenced max 100 feet of movement distance.
4.1.5. Comparison of Doorways Requirements
Table 5
|
Table 5 Doorways Requirements |
||
|
NBC
107: 1994 |
IS
1644:1988 |
OSHA standard,
USA |
|
Open
to a passageway or to the corridor |
Open
to stair way |
Exit
door must be unlocked from the inside only |
|
Not
less than 90cm width |
Not
less than 100cm width |
Able
to open from inside at all times without keys, tools
or special knowledge |
|
180cm
height |
200cm
height |
Side-hinged
exit |
|
Open
outward |
Open
outward |
Must
swing out in the direction of exit travel |
|
No
sliding and overhead door |
Must
be free from signs and decorations. |
|
|
Serve
without key |
Any
doorway that might be mistaken for an exit must be marked "Not an
Exit" or with an indication of its actual use |
|
|
Shall
not immediately open upon stair flight |
||
NBC 107: 1994 has referenced leave entryway will open to section way and open outward toward the path it serves yet the end instrument of leave entryway isn't referenced. These are remembered for IS 16544:1988 and Hong Kong standard individually. Entryway size prerequisite is not exactly different codes which is 90 cm. The Hong Kong Standard has referenced assuming way out entryway open in both manner view board will be given. OSHA standard has referenced leave entryway should be opened from within just consistently without keys, apparatuses, or extraordinary information.
4.1.6. COMPARISON OF CORRIDOR AND PASSAGEWAY REQUIREMENTS
Table 6
|
Table 6 Corridor and Passageway Requirements |
||
|
NBC:107 |
IS
1644:1988 |
OSHA standard,
USA |
|
Not
less than width of exit door |
Width
>=71.1cm (28 inches) at all points |
|
|
Height
of corridor and passageway >=2.4 m |
Height
>= 2.3m (6 feet 8 inches) |
|
|
Any
projection from the ceiling >= 2m (6 feet 8 inches) |
||
It was plainly expressed that exit will open to way however hall and path enumerating were not referenced whereas OSHA has mentioned the standard width, height, and projection from the ceiling at corridor and passageway.
Internal staircase Requirements as expressed only inIS 1644:1988 Ought not be organize around lift with somewhere around one wall on outside wall which should be totally encased without gas funnelling laid in the event that around lift completely encased by material of fire resisting.
There was no arrangement of inner flight of stairs in NBC 107: 1994 and Hong Kong standard. IS 16644: 1988 has referenced that no less than one mass of inward flight of stairs will be on outer wall. It will not orchestrate around lift, whenever organized around lift completely encased by material of fire standing up to.
4.1.7. COMPARISON OF FIRE ESCAPE OR EXTERNAL STAIR REQUIREMENTS
Table 7
|
Table 7 Fire Escape or External Stair Requirements |
||
|
NBC:107 |
IS 1644:1988 |
OSHA standard, USA |
|
Min width
75 cm |
shall
always be directly connected to the ground |
Other
means of escape, such as fire escapes or accessible windows, should be
available where only one exit route is provided. |
|
tread
20 cm |
Entrance
to the external stairs shall be separated and remote from the internal
staircase |
Separated
By Fire Resistant Materials. |
|
riser
height 19 cm |
ensure
that no wall opening, or window opens on to or close to as external stairs |
Must
lead directly outside to a space that is large enough to accommodate all
building occupants likely to use the exit route. |
|
nos.
of riser 15 |
route-
free from obstruction at all times |
|
|
carry
user towards open space |
Min
Width of tread without nosing 30 cm |
|
|
max
height 15 cm |
||
|
nos.
of riser per flight 15 |
||
|
external
stair |
||
|
Not
inclined more than 45 |
||
|
Required
Fire resistance door |
||
NBC 107: 1994 has referenced emergency exit and outside step as single component, though inner break or flight of stairs and outer flight of stairs can have various necessities. Least width of steps, greatest level of riser and least track width were referenced however point of tendency of steps isn't given which was referenced in IS 1644:1988. Specifying of opening in outer wall isn't given in NBC 107:1994.
4.1.8. COMPARISON OF HANDRAIL DETAIL REQUIREMENTS
Table 8
|
Table 8 Handrail Detail Requirements |
||
|
NBC
107: 1994 |
IS
1644:1988 |
OSHA standard,
USA |
|
– |
Height:Min100cm-max 120cm |
must
be at least 28 inches wide at all points between handrails |
|
Gap between
two verticals >=30cm and less than 15cm |
the
exit route must have guardrails to protect unenclosed sides |
|
|
must
be covered if accumulation of snow or ice is likely and is not removed
regularly; |
||
Handrail detail was not referenced in NBC107: 1994 yet specifying of level of handrail was referenced in compositional plan necessities as handrail level will not be under 1000mm Legislature of Nepal (2003). IS 1644:1988 has referenced the necessary level of handrail and hole between two vertical railing.
4.1.9. COMPARISON OF BASEMENT, HORIZONTAL EXIT AND RAMP REQUIREMENTS
NBC 107: 1994 has not referenced cellar and sort of flight of stairs expected for cellar. Though, IS 1644: 1988 has referenced no less than two separate flights of stairs are expected for cellar which might have common path for 15m, and every floor must have 2 staircase access and Hong Kong standard referenced that safeguarded anteroom will be given. The storm cellar steps will be safeguarded more than those over the ground since smoke has inclination to rise. All ways to storm cellar steps will be of smoke control.
NBC 107: 1994 has expressed that exit might prompt another structure yet enumerating for even exit was not referenced. While IS 1644: 1988 has referenced size, entryway and slope important for level exit as 100 cm with at least one fire door of refuse area 0.3m2 /person where Horizontal exit ramp should not be more than 1:10. Doors should be open able from both directions.
NBC 107: 1994 has not mentioned ramp. IS 1644: 1988 had provision of ramp and required gradient as not exceed 1:10 limited to 1:8 and Greater than 1:10 non- slipping material.
4.1.10. COMPARISON OF SIGNS REQUIREMENTS
Signs Requirements in IS 1644:1988 specify as Flush on wall with Floor indication board facing place on wall 0.5m of 0.5m where as in OSHA standard, it is to be posted along the exit route indicating the direction of travel to the nearest exit where the line-of-sight to an exit sign must be uninterrupted and at adult eye-level which should be Self-luminous or electroluminescent with luminance surface value min .06 foot-lambert’s.
NBC 107: 1994 has referenced that signage will be plainly apparent. Position of signage, sign of course to be given and size of signage were not referenced. IS 1644:1988 and Hong Kong standard has referenced size of signage. Directional and leave signs are important to show the area of safeguarded exits and help inhabitants with their way of movement along the leave course (Global Code Board, 200 OSHA standards, USA 9). Without even a trace of sunlight the signs ought to be enlightened so they are noticeable from a good way Malhotra (1993).
Emergency Lighting Requirements in IS 1644:1988 focuses on Emergency lighting and escape lighting. it is well specified in Hong Kong Standards Horizontal lighting 30 lux with combination of natural and artificial lights with backup lighting system.
NBC 107: 1994 and OSHA standard has not referenced crisis light and getaway lighting. While both IS 1644:1998 and Hong Kong standard has arrangement for emergency/ crisis lighting. All getaway courses will be furnished with lighting which comes into activity assuming the typical supplies flop so tenants can find their direction to the safeguarded get away from zones Malhotra (1993).
4.1.11. FIREFIGHTING EQUIPMENT REQUIREMENTS
Table 9
|
Table 9 Firefighting Equipment Requirements |
|
|
NBC
107: 1 |
OSHA standard,
USA |
|
Dry
riser |
Proper
handling and storage. |
|
Wet
riser |
Sprinkles
system |
|
Operable
Alarm system |
|
|
Fire
doors |
|
|
Maintained
exit lighting |
|
|
Portable
fire extinguishers |
|
NBC 107: 1994 has referenced dry and wet riser just, other firefighting devices like smoke alarm, heat locator and alarm were not referenced. Hong Kong standard has arrangement of sprinkle head. During business building studies, it was tracked down dynamic firefighting hardware; smoke alarm, heat locator and so forth assists with advance notice inhabitants and renders fire security of the building (1,2,3,4].
4.1.12. SPECIAL HAZARDS AND EMERGENCY ACTION PLAN REQUIREMENTS
Special Hazards Requirements have been specified by OSHA standard as Holes in roofs or floors, Missing stairs, or steps with unsafe fire escape.
NBC 107: 1994 and IS 1644:1988 has not referenced extraordinary perils. It is a gamble because of risky fire loads, fuel and power supplies or the intensity producing gear. These regions present extra gamble to that related with the structure and in this manner additional safeguards will be taken. It is critical that these regions are detached from the remainder of the convenience for ordinary security. They ought to ideally be found outer to the structure or against an outside wall so passage from outside is conceivable Malhotra (1993).
Maps showing emergency escape routes, Operable employees alarm system, Trained employee in emergency evacuation process and Timely review the emergency action planare provisions in OSHA standard for Emergency Action. it also focuses on job specification by Fixing the person responsible for maintenance of equipment and system.
NBC:107 and IS 1644 has not mentioned the emergency action plan requirements. The Hong Kong Standard has mentioned that the lobby should be protected. Whereas the OSHA has mentioned few more that it must show emergency escape routes, alarm system, trained employee, and timely revision of emergency action plan.
NBC 107: 1994 contains less itemizing when contrasted with IS 1644:1988 and Hong Kong Standard. Flight of stairs assumes a significant part in fire wellbeing; inclination will be given to flight of stairs type and detail. There is no arrangement for plan of steps in building, not referenced where and how the entryway will be put on the step. No arrangement for compressed flight of stairs. Emergency exit and outside step were notice as single component, yet interior break also can go about as an emergency exit. Safeguarded hall and Passageways are essential piece of emergency exit; they lead to extreme spot of wellbeing however no thought has been made in NBC 107: 1994. Firefighting hardware and crisis lighting were not referenced. No subtleties for signs and notice. Level exit and unique danger were not referenced. Necessities for unique dangers and cellar will be given.
5. METHODOLOGY
5.1. STUDY AREA
Bharatpur metropolitan i.e medical city of Nepal having top rated medical institutions in the city, two government’s central hospitals i.e., Bharatpur Hospital and BPKM Cancer Hospital, two Medical Colleges and 25 other private hospitals.
This was assessment research with the aim of studying the fire safety preparedness at the selected hospital buildings in Bharatpur Metropolitan city of Nepal.
Facts of Bharatpur Metropolitan city
Official Name : Bharatpur Metropolitan city
Population : 280502 ( census 2015 )
Location : 84°9’41’’ to 84°29’5’’E & 27°32’58’’to 27°45’40’’N
Altitude range : 140m-390m from sea level.
Temperature : 10°C to 40°C.
Area : 432.95 sq. km
No. of wards : 29
Figure 1

|
Figure 1 Bharatpur Metropolitan city Source Bharatpur Metropolitan city, 2018 |
Selected
Hospitals
Table 10
|
Table 10 Brief Description of Selected Hospital |
||||
|
Features |
BH |
BPKMCH |
CMS |
CMC |
|
Year of Established |
1956 AD |
25th Sep 1999 |
8th Aug 1993 |
2006 AD |
|
Ownership |
Government |
Government |
Private |
Private |
|
No. of Bed |
600 |
500 |
700 |
750 |
|
No. of Building |
4 |
5 |
3 |
1 |
|
Area Covered |
67720 sq m |
81364 sq m |
47404 sq m |
30000 sq m |
Figure 2 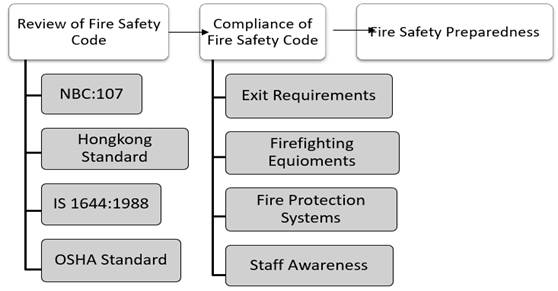
|
Figure 2 Conceptualization of Research Design |
Research design was formulated based on the above concept. Ontological philosophy of research was adopted. It is field based empirical research with descriptive research design. Mixed method research approach was adopted with deductive logical reasoning. Since it was exposed facto research field-based study. Hypothesis wouldn't have been applicable due to lack of control variable. It is duly supported by analysis of codes and literatures.
The purposively sampling was adopted for selecting two public (government) and two private hospitals with relatively similar features in term of level of hospital (center) and bed number (=>500). Two buildings were taken from BH, BPKMCH and CMS whereas one building from CMC was taken for the study. Number of respondents were 32 from each hospital; 2 from different departments of different floor.
The primary data was collected from the field observation of the buildings, questionnaires with staffs, Key Informant interviews. The analytical deductive techniques based on nature of data required were applied. Other tools of primary data collection such as interviewing, discussion with project team and direct observation were also used during field visit.
The main techniques of primary data collection are:
5.4.1. FIELD VISIT AND OBSERVATION
Selected study area was visited in order to analyse the current status of fire safety measures and to understand the compliance status of NBC 107:1994 in selected hospital buildings with different check list.
5.4.2. Questionnaire Survey
Based on the information from the literature review questionnaire has been formulate. Questionnaire was conducted with the staffs at the different wards of selected hospital buildings. This was done to understand fire safety preparedness of hospital building. During questionnaire preparation several references were taken such as Mishra and Shrestha (2017), Lama et al. (2019), Mishra (2019), Mishra and Aithal (2022), Mishra and Aithal (2022), Shah and Mishra (2018), Mishra and Shah (2018), Mishra et al. (2019)and many more.
5.4.3. KEY INFORMANT INTERVIEW
Key informants’ interview was conducted with engineer of consultant to understand the feature of fire safety design and current design practice of hospital building to analyse the exit requirement. Whereas interview was conducted with administration about the evacuation plan of the hospital and with maintenance team about their knowledge, awareness, and drilling skills fire safety management of hospital buildings.
After the collection of data, it was edited and computed for presenting the network diagram, the tables and chart.
5.5.1. DATA COMPILATION AND ANALYSIS
Once the collection of data has been completed, we started to analysis those data. To achieve objective, selected hospital buildings exit places and signage was studied thoroughly, key informant interview was conducted, prepared observation list and data were analysed by qualitative method, staffs respond to the questionnaires was presented in the tables and charts.
Following methods were used
to carry out the data analysis
1) Content Analysis
2) Checklist
3) People’s Perception and Practice on Fire Safety
Descriptive content analysis was carried out for the data obtained from focus group discussion and key informant to document the perception and practice of people about Management of Fire Safety.
6. RESULTS AND DISCUSSION
6.1. COMPLIANCE STATUS OF FIREFIGHTING EQUIPMENT AND FIRE PROTECTION SYSTEMS
To understand the compliance status of fire safety requirement case studies was conducted. Finding from all case studies are summarized below.
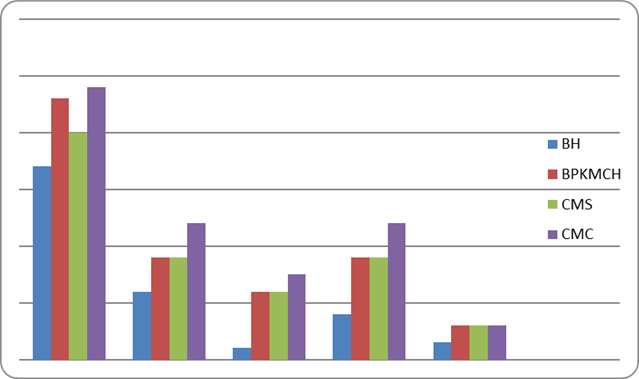
6.1.1. COMPLIANCE STATUS OF AVAILABILITY OF FIREFIGHTING EQUIPMENT
Figure 3
|
Figure 3 Fire Fighting Equipment Available |
The required number of firefighting equipment was not found in the study. So, the total number was counted and compared with each other. Figure 3 reveals that all hospital building had most of the firefighting systems and all lacked the sprinkler system. Bharatpur hospital had less number of firefighting equipment among the selected hospital. Whereas the Chitwan Medical College had highest number among all. The status has somehow similar in commercial building of Birtamode Mishra and Aithal (2022), Lama and Mishra (2022) and Kathmandu Mishra and Shrestha, (2017).
6.1.2. COMPLIANCE STATUS OF AVAILABILITY OF FIRE PROTECTION SYSTEMS
Table 11
|
Table 11 Compliance Status of
Availability of Fire Protection Systems |
||||
|
BH |
BPKMCH |
CMS |
CMC |
|
|
Sprinkler system |
C |
C |
C |
C |
|
Fire detection and alarm system |
B |
B |
B |
B |
|
Emergency lighting |
B |
B |
B |
B |
|
Smoke control system |
C |
C |
C |
C |
|
Riser mains. Hose reels and hydrants |
B |
A |
B |
B |
|
Facilities for the disabled |
B |
A |
B |
A |
|
Fire brigade access and facilities |
A |
A |
A |
A |
|
Fire safety signs and notices |
B |
B |
B |
B |
|
Portable fire Extinguisher |
B |
A |
B |
B |
|
Fire assembly points |
B |
A |
A |
B |
|
Water reservation |
A |
A |
A |
A |
|
Electrical equipment and outlets |
B |
A |
A |
A |
|
Distance from petroleum pump and boiler |
A |
A |
A |
C |
|
Storage of flammable and combustible material |
B |
A |
A |
B |
|
Key: A= sufficient and suitable B= Insufficient
and unsuitable C= Missing and not available |
||||
Table 11 reveals that all four-hospital building’s location was suitable for Fire brigade access and facilities. And all hospitals had sufficient Water reservation. All four hospital buildings were missing Sprinkle system and smoke control system. Only the BPKMCH had met the Riser mains, Hose reels and hydrants requirements. BPKMCH and CMC were found suitable at facilities for the disabled as they had both lift and ramp. Whereas the BH and CMS were found insufficient facilities for the disabled as they had only lifts. All four hospitals had insufficient fire safety signs and notices. Only one hospital was found missing and not available at the distance from petroleum pump i.e., CMC, very near to the petrol pump (within the compound of the hospital). As per the IS code 1644:1988 the petrol pump be placed at distance of minimum 50 meters from the hospital.
6.2. COMPLIANCE
STATUS OF EXIT REQUIREMENTS FOR FIRE SAFETY EVACUATION
6.2.1. COMPLIANCE STATUS OF SELECTED HOSPITALS EXIT ROUTE
Table 12
|
Table 12 Compliance Status of Selected Hospitals Exit
Route |
||||||||||||
|
BH |
BPKMCH |
CMS |
CMC |
|||||||||
|
Exit Route |
E1 |
E2 |
E3 |
E1 |
E2 |
E3 |
E1 |
E2 |
E3 |
E1 |
E2 |
E3 |
|
Free of any obstructions |
Y |
N |
N |
Y |
Y |
Y |
Y |
Y |
N |
Y |
Y |
N |
|
Clearly visible |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Enclosed |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Lead to open space |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
No mirror |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Door locks prohibited |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Permanent |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
E1= Exit 1, E2= Exit 2, E3= Exit 3; Y=Yes, N=No |
||||||||||||
Exit requirements that were compiled in BH were Exit no. 1 met all exit route requirements but Exit no. 2 and 3 are totally or partly covered by aluminium partitions that mean have some obstruction on the way. BPKMCH building Exit no. 1, 2 and 3 met all exit route requirements. CMS building Exit no. 1 and 2 met all exit route requirements. Whereas Exit no.3 route is obstructed by aluminium partitions. CMC building Exit no. 1 and 2 met all exit route requirements. Whereas Exit no.3 route is obstructed by plywoods and old furniture.
6.2.2. COMPLIANCE STATUS OF SELECTED HOSPITALS STAIRCASE
Table 13
|
Table 13 Compliance Status of Selected Hospitals Staircase |
||||||||
|
BH |
BPKMCH |
CMS |
CMC |
|||||
|
Staircase |
S1 |
S2 |
S1 |
S2 |
S1 |
S2 |
S1 |
S2 |
|
Enclosed |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Open
at street |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
N |
|
Min
width 1.5 m |
1.74m |
1.74m |
1.7m |
1.7m |
1.33m |
1.33m |
1.52 m |
1.52 m |
|
Lighting |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Same
no. of stair for each partition |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Separate
stair for fire service |
N |
N |
Y |
Y |
Y |
Y |
Y |
Y |
|
S1= Stair 1,
S2= Stair 2 |
||||||||
BH building staircase were comply with requirements. But they don’t have separate exit route for fire service. BPKMCH building all staircase were complied with the requirements. It also had a separate exit route for fire service. CMS building were not complied with the requirements i.e., the width of the stair_1 was less than the requirement. Whereas they had a separate exit route for fire service. CMC building all staircase were complied with the requirements. It also had a separate exit route for fire service.
6.2.3. COMPLIANCE STATUS OF SELECTED HOSPITALS EXIT DOOR
Table 14
|
Table 14 Compliance Status of Selected Hospitals Exit Door |
||||||||
|
BH |
BPKMCH |
CMS |
CMC |
|||||
|
Exit
Door |
D1 |
D2 |
D1 |
D2 |
D1 |
D2 |
D1 |
D2 |
|
Open
to stair way |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
>=
90 cm width |
209 cm |
160 cm |
280 cm |
170 cm |
220 cm |
170 cm |
120 cm |
120 cm |
|
>=180
cm height |
244 cm |
244 cm |
260 cm |
244 cm |
240 cm |
244 cm |
200 cm |
200 cm |
|
Open
outward |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
No
Sliding and overhead door |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
No
arrange around lift |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Swing
out in the direction of exit travel |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Free
from decorations and signs |
Y |
N |
Y |
N |
Y |
N |
Y |
N |
|
Unlock
from inside only |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Width
of tread >=30 cm |
31 cm |
31 cm |
32 cm |
32 cm |
30 cm |
30 cm |
25 cm |
25 cm |
|
height
of riser <=15cm |
15 cm |
15 cm |
15 cm |
15 cm |
16 cm |
15 cm |
12 cm |
12 cm |
|
Nos.
of stair per flight <= 15 |
9 |
9 |
11 |
11 |
12 |
5/10/2005 |
10 |
10 |
|
D1= Door 1,
D2= Door 2 |
||||||||
BH building Exit Door_1 was complied with all requirements. Whereas Exit Door_2 was not free from decorations. The passage on the staircase had found extra decorations i.e., photo frame and poster of God goddess. BPKMCH building Exit Door_1 was complied with all requirements. Exit Door_2 was found not free from decorations and number of stairs was found not equal. The passage on the staircase had found extra decorations i.e., photo frame and poster of God goddess. CMS building Exit Door_1 and Exit_2 were found not complied with all requirements. In Exit Door_1 the height of the riser was higher than requirement. Exit Door_2 was not free from decorations and the number of stairs was not same as per NBC 107:1994 and IS 1644:1988. CMC building ExitDoor_1 was found complied with all requirements. Exit Door_2 was not free from decorations. The passage on the staircase had found extra decorations i.e., photo frame and poster of God goddess.
6.2.4. COMPLIANCE STATUS OF SELECTED CORRIDOR AND PASSAGEWAY
Table 15
|
Table 15 Compliance Status of Selected Corridor and Passageway |
||||||||
|
BH |
BPKMCH |
CMS |
CMC |
|||||
|
Corridor
and passageway |
P1 |
P2 |
P1 |
P2 |
P1 |
P2 |
P1 |
P2 |
|
>=2.4
m height |
3.58 m |
3.58 m |
3.3 m |
3.3 m |
2.7 m |
2.7 m |
5.4 m |
5.4 m |
|
>=71.1
cm width |
340 cm |
340 cm |
190 cm |
190 cm |
220 cm |
220 cm |
350 cm |
320 cm |
|
P1= Passage
1, P2= Passage 2 |
||||||||
On the observation of the selected hospital buildings, it was found that all hospitals were complied with the standards
6.2.5. COMPLIANCE STATUS OF SELECTED HOSPITALS EXTERNAL STAIR
Table 16
|
Table 16 Compliance Status of Selected Hospitals External Stair |
||||
|
BH |
BPKMCH |
CMS |
CMC |
|
|
External stair |
Stair1 |
Stair1 |
Stair1 |
Stair1 |
|
Lead
to an open space enough to the building occupants |
Don’t
have external stair |
Y |
Y |
Y |
|
Separate
entrance and remote from internal staircase |
Y |
Y |
Y |
|
|
Separated
by fire resistant material |
Y |
Y |
Y |
|
BPKMCH, CMS and CMC buildings had external stair and they were complied with the requirements whereas BH buildings didn’t have external stair.
6.2.6. COMPLIANCE STATUS OF SELECTED HOSPITALS HANDRAIL
Table 17
|
Table 17 Compliance Status of Selected Hospitals Handrail |
||||||||
|
BH |
BPKMCH |
CMS |
CMC |
|||||
|
Handrail |
Exit 1 |
Exit 2 |
Exit 1 |
Exit 2 |
Exit 1 |
Exit 2 |
Exit 1 |
Exit 2 |
|
>=100 cm height |
90 cm |
90 cm |
104 cm |
104 cm |
84 cm |
84 cm |
100cm |
100cm |
|
<= 28-inch gap between two
vertical |
7.5 inch |
7.5 inch |
22 inch |
22 inch |
16inch |
16inch |
22inch |
22inch |
In the study the following facts were found. BH buildings, the height of the handrail is shorter than the requirement. BPKMCH buildings, the handrail were complied with the requirements. CMS buildings, the height of the handrail was shorter than the requirement whereas CMC buildings, the handrail were complied with the requirements.
6.2.7. COMPLIANCE STATUS OF SELECTED HOSPITALS RAMP
Table 18
|
Table 18 Compliance status of Selected Hospitals Ramp |
||||||
|
BH |
BPKMCH |
CMS |
CMC |
|||
|
Ramp |
Exit 1 |
Exit 1 |
Exit 2 |
Exit 1 |
Exit 1 |
Exit 2 |
|
1:8 to 1:10 slop |
Don’t have Ramp |
1:10 |
1:10 |
Don’t have |
1:10 |
|
|
Non-slipping material |
Y |
Y |
Y |
|||
|
Enclosed |
Y |
Y |
Y |
|||
In the study the following facts were found. BH buildings didn’t have a Ramp. Whereas there was a ramp under construction between Block A and C. BPKMCH buildings were complied with the ramp requirements. CMS buildings didn’t have a Ramp and had four lifts in a building. CMC buildings were complied with the requirements.
6.2.8. COMPLIANCE STATUS OF SELECTED HOSPITAL BUILDINGS SIGNS
Table 19
|
Table 19 Compliance status of Selected Hospital buildings Signs |
||||||||
|
BH |
BPKMCH |
CMS |
CMC |
|||||
|
Signs |
E 1 |
E 2 |
E 1 |
E 2 |
E 1 |
E 2 |
E 1 |
E 2 |
|
Proper
signage |
N |
N |
N |
N |
N |
Y |
N |
N |
|
Visible |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
|
Illuminate |
N |
N |
Y |
Y |
Y |
Y |
Y |
Y |
|
Floor
indication board 0.5 m X 0.5 m |
N |
N |
Y |
Y |
Y |
Y |
Y |
Y |
|
Height
at adult eye-level |
Y |
Y |
Y |
N |
Y |
Y |
N |
Y |
|
Arrow
to way |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
|
E1= Exit 1, E2=
Exit 2 |
||||||||
In the study the following facts were found. BH: It had very few numbers of signs, all are not illuminated and didn’t find floor indication board. BPKMCH: It had very few numbers of signs. CMS: It had very few numbers of signs. CMC: It had very few numbers of signs. And the signs are not at eye level
6.2.9. COMPLIANCE STATUS OF SELECTED HOSPITALS BUILDING OCCUPANCY
Table 20
|
Table 20 Compliance Status of Selected Hospitals Building Occupancy |
|||||||
|
BH |
BPKMCH |
CMS |
CMC |
||||
|
Building
Occupancy |
E 1 |
E 2 |
E 1 |
E 2 |
E 1 |
E 2 |
E 1 |
|
Decreasing
toward exit discharge path |
Y |
Y |
Y |
Y |
Y |
Y |
Y |
In the study the following facts were found. BH: The status of the building occupancy was complied with the requirements. BPKMCH: The status of the building occupancy was complied with the requirements. CMS: The status of the building occupancy was complied with the requirements. CMC: The status of the building occupancy was complied with the requirements.
6.3. AWARENESS
OF STAFFS ON FIRE SAFETY OF SELECTED HOSPITAL BUILDING
To understand the compliance status of Awareness of the staffs on fire safety of Staffs of Selected Hospital Building
Figure
4
|
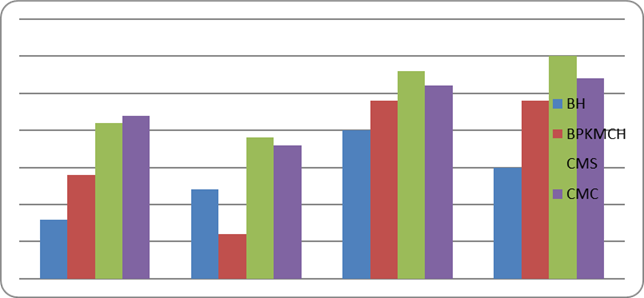
Figure 4 Awareness of Building Feature |
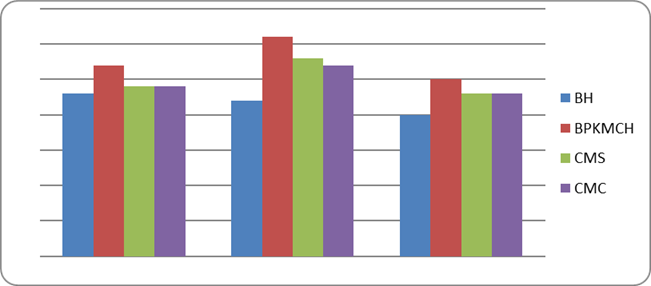
The Figure 4 shows the awareness of staff on Hospital Building features. At Bharatpur hospital 71.9% of respondents know the building design, 68.8% of respondents can locate the exits and for 62.5% emergency sign were visible. At BPKMCH 84.4% of respondents know the building design, 96.7% of respondents can locate the exits and for 78.1% emergency sign were visible. At CMS 75% of respondents know the building design, 87.5% of respondents can locate the exits and for 71.9% emergency sign were visible. At CMC 75% of respondents know the building design, 84.3% of respondents can locate the exits and for 71.9% emergency sign were visible. Figure 4.2 revealed that most of the staff were found aware on building feature.
Figure 5
|
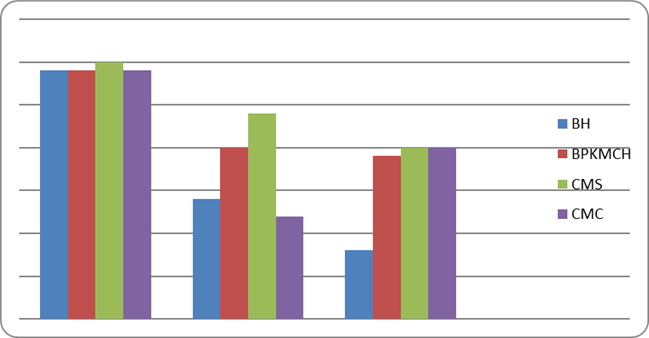
Figure 5 Awareness on Emergency Egress |
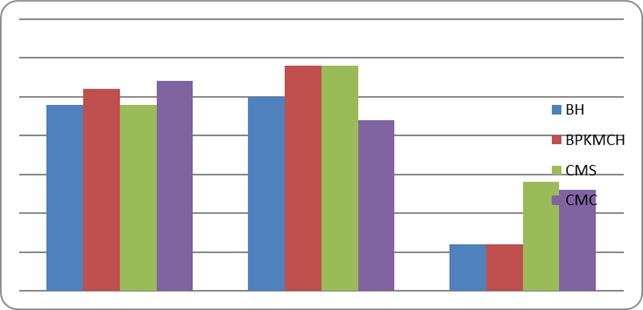
The Figure 5 shows the awareness of staff on Emergency Egress. At BH 75% of respondents were aware on emergency evacuation, 78.1% of respondents can find the assembly point and 18.9% of respondents only had attained the evacuation training. At BPKMCH 81.2% of respondents were aware on emergency evacuation, 90.6% of respondents can find the assembly point and 18.9% of respondents only had attained the evacuation training. At CMS 75% of respondents were aware on emergency evacuation, 90.6% of respondents can find the assembly point and 43.7% of respondents only had attained the evacuation training. At CMC 84.4% of respondents were aware on emergency evacuation, 68.8% of respondents can find the assembly point and 40.6% of respondents only had attained the evacuation training.
Figure 6
|
Figure 6 Awareness on Emergency Procedure |
The Figure 6 shows the awareness of staff on Emergency Procedure. At BH 25% of respondents were aware about provision of fire-alarm, 37.5% of respondents were found aware about the instruction to flow when alarm is sounded, 62.5% of respondents had contact person's details and 46.9% of respondents had important phone number list. At BPKMCH 62.5% of respondents were aware about provision of fire-alarm, 18.9% of respondents were found aware about the instruction to flow when alarm is sounded, 75% of respondents had contact person's details and 75% of respondents had important phone number list. At CMS 65.5% of respondents were aware about provision of fire-alarm, 59.4% of respondents were found aware about the instruction to flow when alarm is sounded, 87.5% of respondents had contact person's details and 93.7% of respondents had important phone number list. At CMC 68.8% of respondents were aware about provision of fire-alarm, 56.2% of respondents were found aware about the instruction to flow when alarm is sounded, 81.2% of respondents had contact person's details and 84.3% of respondents had important phone number list.
Figure
7
|
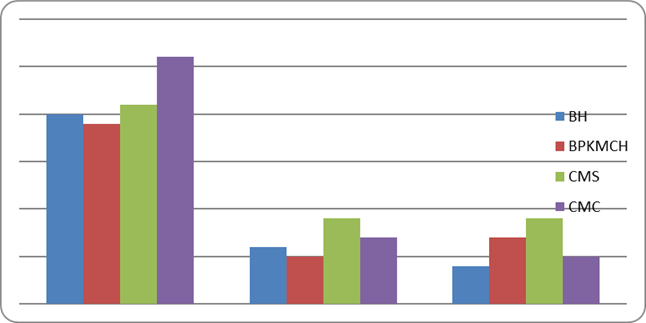
Figure 7 Awareness on Fire Safety Measures |
The Figure 7 shows the awareness of staff on Fire Safety Measures. At BH 90.6% of respondents were found known about fire extinguisher, 43.7% of respondents were found known about Water hose reel and only 25% of respondents were found known about Fire hydrant. At BPKMCH 90.6% of respondents were found known about fire extinguisher, 62.5% of respondents were found known about Water hose reel and 59.4% of respondents were found known about Fire hydrant. At CMS 93.7% of respondents were found known about fire extinguisher, 75% of respondents were found known about Water hose reel and 62.5% of respondents were found known about Fire hydrant. At CMC 90.6% of respondents were found known about fire extinguisher, 46.9% of respondents were found known about Water hose reel and 59.4% of respondents were found known about Fire hydrant.
Figure 8
|
Figure 8 Awareness to Operate Fire Equipment |
The Figure 8 shows the awareness of staff to operate Fire Equipment. At BH 62.5% of respondents had ability to operate fire extinguisher, 18.9% of respondents had ability to operate Water hose reel and only 12.5% of respondents had ability to operate Fire hydrant. At BPKMCH 59.4% of respondents had ability to operate fire extinguisher, 28.1% of respondents had ability to operate Water hose reel and only 21.8% of respondents had ability to operate Fire hydrant. At CMS 65.6% of respondents had ability to operate fire extinguisher, 28.1% of respondents had ability to operate Water hose reel and 28.1% of respondents had ability to operate Fire hydrant. At CMC 81.2% of respondents had ability to operate fire extinguisher, 21.8% of respondents had ability to operate Water hose reel and only 15.6% of respondents had ability to operate Fire hydrant.
7. CONCLUSION
Different articles were reviewed regarding exit requirements for fire safety at hospital buildings and found missing the specific guidelines for fire safety at hospital building, however the OSHA standards had explained few. NBC had explained all about commercial building code and lacked specific guideline for hospital buildings. Where the hospital buildings are more sensitive, so monitoring of the required guidelines at during construction and post construction would enhance the hospital safety.
From the findings, it was revealed that fire safety preparedness was not a priority in the selected hospital buildings. They lacked on firefighting equipment such as smoke detector, heat detector, fire alarm, water hose reel. And they all missed the water sprinkle. Private and public hospitals, almost all of them reveal the same level of preparedness. The hospital governed by government; Bharatpur Hospital had fewer of firefighting equipment.
The selected hospital had inadequate fire protection system in place. All four hospitals were found located at suitable fire brigade access facilities and also had sufficient water reservation. Both government hospitals and one private hospital (CMS) had sufficient assembly point area, whereas the private hospital CMC had missing assembly point. They all had insufficient fire safety signs and notices. BH, BPKMCH and CMS were located at suitable distance from petroleum pump and boiler, whereas the private hospital CMC was unsuitable at distance from petroleum pump. It was also investigated that all four hospitals were found missing smoke control system and sprinkler system.
All the selected hospital buildings exit route and doors were found permanent, enclosed, clearly visible and had no mirror. One exit door of CMC was found not leading to open space. Some obstructions of plywood, aluminum bar and furniture were found at BH, CMS and CMC, whereas the BPKMCH had found free of obstructions. The government hospital BH was found not compliance many statuses of exit requirement. The exit route was found obstructed by aluminum partitions, not free from decorations, didn’t have separate stair for fire service, missing ramp, and no proper signage. However, the government hospital BPKMCH was found more prepared for fire safety as it was found compliance in the status of exit requirements.
All selected hospital’s staff were found aware about the general feature of the building like building plan, location for exit and assembly points. It was also found that many of the staffs of all selected hospital were not trained for emergency evacuation. They lacked awareness on emergency procedure as they had not enough alarm system, staffs were found self-prepared for the instruction to follow for alarm. Even they lacked the list of important phone number list. It was found that the staff had only internal person’s details, most of the staffs had only intercom phone number list.
None of the hospital had a comprehensive emergency plan in place, insufficient awareness of availability of firefighting equipment and ability to operate them. Most of the staffs had ability to operate only fire extinguisher. In comparing to the government hospital, the private hospital’s staffs were found more aware on fire safety measures and also, they were more capable to operate fire equipment. Regular training and fire drill practices were found missing.
8. RECOMMENDATIONS
The subsequent points can be recommended:
All the exit requirements should be strongly enforced in all hospital buildings.
1) Emergency procedure including important phone number list should be enforced tin practice in all hospitals.
2) All hospital should manage all firefighting equipment and fire protection system as required.
3) Awareness about equipment and fire drill practice should be regularly conducted.
4) Fire safety department and team should be formed, and responsibility be entrusted.
5) An emergency manual should be prepared and implemented in collaboration with the Ministry of Health and Population, Disaster Management Department (Ministry of Home and Affair) and local government.
6) The fire safety preparedness program should be mainstreamed into the health plans of the ministry of health and population to enable health practitioners understand how to avoid and respond to fire incidents.
7) Fire safety design should be approved by fire authority and monitored properly.
8) Fire authority should inspect the firefighting infrastructure and impose the strict regulation for adaptation.
9) Emergency education and awareness programs should be part of training and retraining of health personnel.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
The author is thankful to all the key informants and hospital staff and management for helping in collecting data.
REFERENCES
Adpc-Asian Disaster Preparedness Centre (2000). Project Completion Report : Kathmandu Valley Earthquake Risk Management Program (KVERMP), Adpc, Bangkok, Thailand American Journal of Disaster Medicine, 3(1), 5-14.
Baker, J. (2013). The Relationship Between Fire Damage and Fire Safety Management, MPhil. Lounghborough University.
Bartley, B. H., Stella, J. B., and Walsh, L. D. (2006). What A Disaster ?! Assessing Utility of BPIKHS-B.P. Koirala Institute of Health Sciences, 2007, Disaster Response Plan, BPKIHS, Dharan, Nepal.
Bartley, B. H., Stella, J. B., And Walsh, L. D. (2006). What A Disaster ?! Assessing Utility of Simulated Disaster Exercise and Educational Process for Improving Hospital Preparedness. Prehospital and Disaster Medicine, 21(04), 249-255. https://doi.org/10.1017/S1049023X00003782.
Bradt, D. A., And Drummond, C. M. (2007). Professionalization
of Disaster Medicine-an Appraisal of Criterion-Referenced Qualifications.
Pre-Hospital and Disaster Medicine, 22(5), 360-368. https://doi.org/10.1017/S1049023X00005069.
Building Department (2011). Code of Practice for Fire Safety in Buildings.
Buildings at Birtamode, Jhapa, Nepal. J Adv Res.
Burger, E. (2007). Preparing An Orthopedic Practice to
Survive A Natural Disaster: A Retrospective Analysis of Rebuilding After
Hurricane Katrina. Orthopedics, 30(4), 290. https://doi.org/10.3928/01477447-20070401-13.
Chokshi, N. K., Behar, S., Nager, A. L., Dorey, F., and Upperman, J. S. (2007). Disaster Management Among Pediatric Surgeons : Preparedness, Training and Involvement. https://doi.org/10.5055/ajdm.2008.0001.
Const Urban Arch (2022). 7(3-4), 1-16.
Derek, J. (1986). Fire Prevention Handbook. London : Butterworth and Company (Publishers) Limited.
Dhruba, G. A. (2011). Need and a Capacity Assessment of Fire Preparedness in the Municipalities of Nepal.
Drabek, T. (1986). Human System Responses to Disaster: An Inventory of Sociological Findings. Springer Verlag, New York. https://doi.org/10.1007/978-1-4612-4960-3.
Fire Safety (2017). The Science and its Application to Building Codes, Canada : NRC [Online].
Gebbie, K., And Qureshi, K. (2006). A Historical Challenge :
Nurses and Emergencies. OJIN : The Online Journal of Issues in Nursing, 11(3). https://doi.org/10.3912/OJIN.Vol11No03Man01.
Irene K., David B., Miranda M, and Harrlet C., (2009). Emergency Preparedness.
Lama, S. and Mishra, A. K. (2022). Operational Assessment of Fire Safety Status of Existing Commercial Buildings at Birtamode, Jhapa, Nepal. https://doi.org/10.5281/zenodo.7222816
Lama, C., Sah, D.P. and Mishra, A.K. (2019)."Occupational
Hazards Identification and Their Risk Assessment During The Construction of
Head Race Tunnel in Middle Bhotekoshi Hydroelectric Project."
International Journal of Research -Granthaalayah, 7(3), 227-248. https://doi.org/10.29121/granthaalayah.v7.i3.2019.965.
MOH/WHO/NSET, Kathmandu, Nepal.
Ma, Q., and Huangt, T. (2011). Analysis of And Study on the Difficulties
in the Fire Protection Design of Large Commercial Complex. in : Procedia
Engineering, The 5th Conference on Performance-Based Fire and Fire Protection
Engineering. Tianjin, China. Elsevier Ltd. https://doi.org/10.1016/j.proeng.2011.04.661.
Malhotra, H.L. (1993). Fire Safety in Buildings.
Martyn, Y. et al. (2020). Software for Shelter's Fire Safety
and Comfort Levels Evaluation Data Stream Mining and Processing, 1158. https://doi.org/10.1007/978-3-030-61656-4_31.
Mehaffey, J. R. (1987). Flammability of Building Materials and Fire Growth, Designing for Fire Safety : The Science and its Application to Building Codes.
Ministry of Health and Family Welfare (2010). A First Line Maintenance Guide for End Users, New Delhi.
Ministry of Home Affairs. (2018). Nepal Disaster Report, 2017 : The Road to Sendai, Kathmandu, Government of Nepal.
Ministry of Home Affairs/Disaster Summery.
Mishra,
A. K., and Aithal, P. S. (2022). Preparedness and Costing on Fire Safety
Installationin Commercial Buildings. International Journal of Applied
Engineering and Management Letters (IJAEML), 6(2), 182-196. https://doi.org/10.5281/zenodo.7108648.
Mishra, A.K. (2019). Housing Needs Fulfillment For Low -Income
Group, Livas: International Journal on Livable Space, 4(2), 40-47. http://dx.doi.org/10.25105/livas.v4i2.5630.
Mishra, A.K. and Aithal, P.S. (2021). Techno-Legal
Provisions for Safer High-rise Apartment Construction in Nepal. J Adv Res Geo
Sci Rem Sens 8(1), 16-46.
https://doi.org/10.24321/2349.7661.202102.
Mishra, A.K. and Shrestha, A. (2017). Assessment of Exit Requirements for Fire Safety of Commercial Buildings, Kathmandu, Nepal. International Journal of Emerging Technologies and Innovative Research, 4(10), 248-255.
Mishra, A.K. and Shrestha,
A. (2017). Fire Safety
Preparedness Among Occupants
of Selected Commercial Buildings, Kathmandu,
Nepal, 5(4), 1-13.
Mishra, A.K. and Shrestha,
A. (2017). Assessment of Exit Requirements for Fire Safety of Commercial Buildings, Kathmandu,
Nepal, 4(10),1-8.
Mishra, A.K., Lama, C., and Sah, D.P. et al. (2019).
Effectiveness of Safety Measures Implementation. J Adv Res Civil Enviengr,
6(2), 1-20. https://doi.org/10.24321/2393.8307.201903.
Mishra, A.K., and Shrestha, A. (2017). Fire Safety Preparedness Among Occupants of Selected Commercial Buildings, Kathmandu, Nepal. International Journal of Creative Research Thoughts, 5(4), 195-207.
Mishra, A. K., and Shah, S.K. (2018). Estimating Housing Unit for Low Income Group of People in Kathmandu, Nepal. NOLEGEIN Journal of Operations Research and Management, 1(2). https://doi.org/10.37591/njorm.v1i2.185.
Mitigation in Health Facilities, PAHO/WHO, Washington D. C.
MoHA-Ministry of Home Affairs (2004). Disaster Scenario of Nepal, Moha, Government of Nepal.
NSET-National Society for Earthquake Technology-Nepal, (2004). Final Report on Disaster Inventory/Information Management System in Nepal, NSET, Kathmandu, Nepal.
Nepal National Building Code (1994). NBC107 : 1994. Provisional Recommendation on Fire Safety (May).
Ogajo, N. J., (2013). Influence of Fire Disasters on Mitigation and Preparedness in Commercial Premises in Kenya, A Survey Study of Kisumu CBD. B.A. School of Built Environment, University of Nairobi.
PAHO-American Health Organization and WHO-World Health Organisation (2004). Principles of Disaster Mitigation in Health Facilities, PAHO/WHO, Washington D. C.
PAHO-American Health Organization and WHO-World Health Organisation (2005). Safe Hospitals: A Collective Responsibility, PAHO/WHO, Washington D. C.
Pan American Health Organization. Hospital Fire Prevention and Evacuation Guide. (2014).
Patan Hospital, (2005). Disaster Plan of Patan Hospital, Patan Hospital, Lalitpur, Nepal.
Practices For People With Disabilities Analysis of Some Current Practices and Preparedness. Prehospital And Disaster Medicine, 21(04), 249-255.
Recommendations for Future Training Programs. Journal of Disability Policy Studies, 17(4), 216-222.
Rowland, J. L., White, G. W., Fox, M. H., and Rooney, C. (2007). Emergency Response Training.
Rowland, J. L., White, G. W., Fox, M. H., and Rooney, C. (2007). Emergency Response Training Practices for People With Disabilities Analysis of Some Current Practices and Recommendations for Future Training Programs. Journal of Disability Policy Studies, 17(4), 216-222. https://doi.org/10.1177/10442073070170040401.
Shah, S. and Mishra, A.K., (2018). Review on Global Practice
of Housing Demand Fulfilment for LowIncome Group People. NLEGEIN Journal of
Business Ethics, Ethos and CSR, 1(2), 5-16. https://doi.org/10.37591/njbeec.v1i2.187.
Technology-Nepal (2004). Non-Structural Vulnerability Assessment of Hospitals in Nepal.
The Joint Commission (2008). Guiding Principles for the Development of the Hospital of the Future.
UNDP. (2009). Recommendation for Update of Nepal National Building Code. Kathmandu, Nepal : United Nation Development Program (UNDP).
UNDP/BCPR-Bureau for Crisis Prevention and Recovery, (2004). Reducing Disaster Risk : A Challenge for Development, UNDP.
UNDP/UNCHS-Habitat (1994). Seismic Hazard Mapping and Risk Assessment for Nepal, UNDP Nepal USAID and NSET-National Society for Earthquake Technology-Nepal, (2009) Hospital Preparedness for Emergency (HOPE) Course : Instructor Work Book, USADID/NSET
Wisconsin Hospital (2004). Wisconsin Hospital Emergency Preparedness Plan, Wisconsin Hospital.
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2022. All Rights Reserved.

