EPIDEMIOLOGY OF DOWN’S SYNDROME & Β- THALASSEMIA IN INDIANilima Gajbhiye 1 1 Associate Professor, Department of Life Science, Ramnarain Ruia Autonomous College, Mumbai-19(M.S.), India2 Post graduate student, Department of Life Sciecnce, Ramnarain Ruia Autonomous College, Matunga, Mumbai-19(M.S.), India |
|
||
|
|
|||
|
Received 26 January 2022 Accepted 27 February 2022 Published 10 March 2022 Corresponding Author Nilima Gajbhiye, drneem@yahoo.com DOI 10.29121/granthaalayah.v10.i2.2022.4515 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2022 The
Author(s). This is an open access article distributed under the terms of the
Creative Commons Attribution License, which permits unrestricted use, distribution,
and reproduction in any medium, provided the original author and source are
credited.
|
ABSTRACT |
|
|
|
Down’s syndrome and
Beta (β) Thalassemia are commonly
prevalent genetic diseases worldwide.
Down’s syndrome is predominantly caused by an extra copy of chromosome 21 or trisomy 21. Maternal age above 35
years significantly increases the chances of a Down’s syndrome birth. In India, there are approximately 21,000
Down’s syndrome births every year.
β-Thalassemia is a blood disorder caused by abnormal synthesis of the
β chains of hemoglobin. India
has over 35-45 million carriers of this disease. This is a survey-based study,
which aims to understand the epidemiology of Down’s syndrome and Beta Thalassemia in the Indian population.
This online survey was answered by 297 Indian or Indian origin adults. Both females and males were the
respondents. Results of the study indicated
that prevalence of Down’s syndrome is low in India while that of
β-thalassemia is moderate.
The correlation between the maternal and paternal ages at the time of birth
of a Downs syndrome affected person
was determined and the analyses showed that there was a positive correlation. |
|
||
|
Keywords: Epidemiology, Survey, Down’s Syndrome, Thalassemia, Trisomy, Maternal
Age 1. INTRODUCTION
Down’s Syndrome, also known as Trisomy-21, is the most prevalent
genetic disease worldwide Kazemi et al. (2016). There are three cytogenetic forms of Down’s
Syndrome- free/non-disjunction trisomy 21, mosaic trisomy 21 and Robertsonian
translocation trisomy 21 Plaiasu (2017). The phenotypic features of Down’s syndrome result
from dosage imbalance of genes located on chromosome 21. The common features
of Down’s syndrome are mental retardation, craniofacial abnormalities, atrioventricular
septal defects (AVSD), acute leukemia, gastrointestinal problems, small
cerebral and cerebellar hemispheres, and brainstem. Individuals affected with
Down’s syndrome have a variety of physical features like a small chin,
slanted eyes, poor muscle tone, a flat nasal bridge Asim et al. (2015), epicanthal skin folds in the upper eyelid that
forms a layer of skin covering the inner corner of the eye and below-average
height. Mental retardation is the most common symptom of this disease Verma et al. (2012). Maternal age above 35 years increases the chances
of a Down’s syndrome birth as the probability of non-disjunction increases
with the length of the time the primary oocyte is in the ovary Russell (n.d.). The average life expectancy in developed countries
is 55 years Asim et al. (2015). The incidence reported worldwide is 1 in 700 to 1
in 800 live births Kava et al. (2004). In India, approximately 21,000 babies are born with Down’s
syndrome every year, with the majority of cases
being identified postnatally Kava et al. (2004) Beta (β) |
|
||
Thalassemia is a group of hereditary blood disorders caused by abnormal synthesis of β chains of haemoglobin Galanello and Origa (2010). β-thalassemia is an autosomal recessive disorder Hassan et al. (2016).
Approximately 1.5% of the global population (80 to 90 million people) being carriers of the disease and about 60,000 symptomatic individuals being born annually Galanello and Origa (2010). Beta-thalassemia includes three main forms: Thalassemia Major, Thalassemia Intermedia and Thalassemia Minor (also called beta-thalassemia carrier/beta-thalassemia trait). Individuals with β- thalassemia major are homozygotes for beta0 or beta+ genes characterized by two defective genes, leading to no synthesis of β-globin. These individuals have a severe form of disease requiring lifelong transfusion and may have shortened life span Wahed and Dasgupta (2015).Individuals with Thalassemia intermedia have two defective genes, but some β-globin production is observed in these individuals, having mild anaemia, and only occasionally requiring transfusion Wahed and Dasgupta (2015). Carriers of thalassemia minor are mostly heterozygotes and are usually asymptomatic, sometimes having mild anaemia. β-Thalassemia minor is the most common form of β- thalassemia Cao and Galanello (2010). When both parents are carriers there is a 25% risk of having children with severe thalassemia Galanello and Origa (2010). Β-thalassemia is the most common single-gene disorder in the Indian population Grow et al. (2014), with over 10% of the total world thalassaemic being born in India every year Bashyam et al. (2004).India has over 35-45 million β-thalassemia carriers Colah et al. (2017). β-thalassemia is more prevalent in India than its counterpart α-thalassemia as severe alpha deletion mutations are less common in the Indian region Panigrahi and Marwaha (2007). Certain communities in India, like Sindhis, Gujaratis, Punjabis, and Bengalis, are more commonly affected with β-thalassemia Gupta et al. (2015). The most common mutation found in the β-globin gene is the IVS1-5(G→C) mutation (Anju Gupta et al., 2003), with a national prevalence of 56.3% in India, 64.6% in Sri Lanka and 36.5% in Pakistan Black et al. (2010).
The aim of this study was to determine the epidemiology of Down’s syndrome and Beta- thalassemia in the Indian population. The objective of this study is to understand the prevalence of these two diseases in India which will help raise awareness about them.
2. MATERIALS AND METHODS
The study was carried out by the survey-based method. A survey formulated on Google Forms was circulated through the messaging platform WhatsApp. The survey was answered by 297 adults. Majority were from the state of Maharashtra. The present study was conducted in accordance with the declaration of Helsinki. The consent was taken from all participants involved in the study.
Inclusion Criteria: In this survey, men, and women in the age group of 18 years to 90 years were included. All participants were Indians or of Indian origin. For surveying Down’s syndrome, the persons were to give the information of some family member suffering from the disease considering the physical constraints of a Down’s syndrome patient.
Exclusion Criteria: All persons below age of 18 years were excluded.
Statistical Analysis: The data obtained from the survey was analysed by online statistical software MS Excel. The tools of analysis used were Student’s t-test & Karl Pearson’s Correlation Coefficient to determine the relationship between various factors in the survey.
3. RESULTS AND DISCUSSION
3.1. DOWN’S SYNDROME
Out of the 297 respondents, seven persons had a history of Down’s syndrome in their family. All the seven cases were diagnosed after birth of the child.
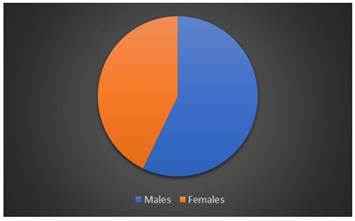
The gender distribution of Down’s syndrome was not skewed drastically towards any sex in general with the number of male patients being marginally higher than the number of females patients.
|
|
|
Figure 1 Gender Distribution of Down’s
Syndrome |
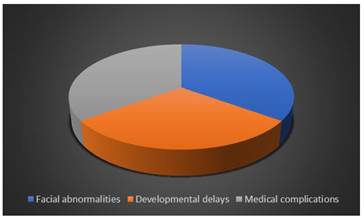
All the seven patients had complications related to Down’s syndrome such as facial abnormalities, developmental delays, and medical complications.
|
|
|
Figure 2 Complications
associated with Down’s syndrome |
Correlation analysis was performed to determine the relationship between the maternal and paternal ages at the time of birth of the Down’s syndrome patients. The value of Karl Pearson’s correlation coefficient obtained was 0.962087 which indicated a strong positive correlation between the two variables. Thus, higher the ages of both mother and father at the time of birth, higher was the risk of the child having Down’s syndrome.
The results of this study showed that the prevalence of Down’s syndrome is very low in India. Due to the wide diversity in demographics and ethnicity in India, there are different prevalence rates for Down’s syndrome throughout the country Al-Biltagi (2015). In a study conducted in Kozhikode district of Kerala, 66 cases out of the 274 cases studied were diagnosed with Down’s syndrome, with the mean maternal age estimated to be 30.34 years and mean paternal age to be 31.04 years, which is in contrast to the normal accepted fact that occurrence of Down’s syndrome increases with increase in maternal age Aparnna and Jose (2014). But our study showed that there was a positive correlation between the higher maternal and paternal ages and the risk of conceiving a baby with Down’s syndrome that is consistent with the general findings from other studies Sherman et al. (2007), Eggermann and Schwanitz (2011), Pankaj et al. (2015) Mental retardation is the most common symptom associated with this disease as indicated in our study Verma et al. (2012).No information was obtained about the connection of Down’s syndrome to the habits of a person like smoking, alcohol consumption, contraceptive pills consumption etc, although consuming tobacco and oral contraceptives are a significant risk factor for down’s syndrome birth, with tobacco use primarily a risk factor in younger women and oral contraceptive use primarily a risk factor in older women Ghosh et al. (2011).
3.2. BETA THALASSEMIA
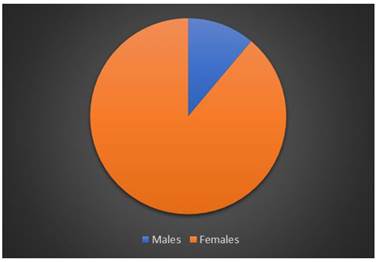
Out of the 297 respondents, nine persons had β- Thalassemia. The gender distribution of the respondents for this disease were overwhelmingly female with only one out of the nine respondents being male.
|
|
|
Figure 3 Gender Distribution of
β-Thalassemia |
Of the nine respondents, six were from Maharashtra, two from Goa and one from Gujarat. The type of β-Thalassemia observed in this survey was mainly the Minor type with only two respondents having β-Thalassemia Major. No case of β-thalassemia Intermedia was reported. Five out of the nine persons had a family history of the disease.
|
|
|
Figure 4 Distribution
of the Type of Beta Thalassemia |
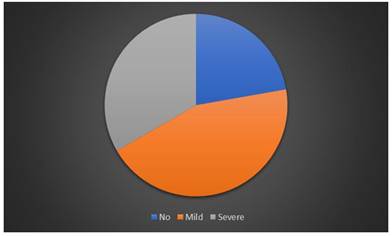
The observations of anaemia among the respondents were varied with most of them having mild anaemia. Only the two respondents with β-Thalassemia major had severe anaemia.
|
|
|
Figure 5 Distribution of anemia in the respondents |
All the respondents who were β-Thalassemia minor did not take any treatment for it, while the two respondents who were β-Thalassemia major had to undergo blood transfusions every 15 days in addition to taking iron chelation tablets.
β-thalassemia is found to be moderately prevalent with the minor type of the disease accounting for majority of the cases, suggesting that β-thalassemia minor was more common in India as noticed in previous studies Shah et al. (2017), Mohanty et al. (2013) The patients with the major type of the disease had to undergo blood transfusions as established in previous findings Aldemir (2018).
4. CONCLUSION AND RECOMMEDATIONS
The prevalence was Down’s syndrome was found to be low in the Indian population as only 7respondents had a family history of the disease. Very less data was obtained about the disease as people may not be aware of the age of diagnosis and the age of the parents at time of birth of the affected child. The patient may not have been closely related to them. Albeit the correlation between the maternal and paternal age at the time of birth of the affected child was determined, and a positive correlation was observed. No information was obtained about the connection of Down’s syndrome to the lifestyle and habits of a person like smoking, alcohol consumption, contraceptive pills consumption etc.
β-Thalassemia was found to moderately prevalent in the Indian population with majority of the respondents having β-Thalassemia minor. There may have been more cases of the disease among the respondents as some who have the minor variant may not be aware that they have the disease. Among the respondents, anaemia was not observed as major symptom, the exceptions being the two β-Thalassemia major respondents.
The information obtained in the present survey can aid in the understanding of the occurrence and prevalence of the two diseases in India as well as increase the awareness of people for the signs and symptoms of the diseases.
REFERENCES
Al-Biltagi, M. (2015) Cronicon PAEDIATRICS Down syndrome from Epidemiologic Point of View. Retrieved from https://www.researchgate.net/profile/Mohammed-Al-Biltagi/publication/281783735_Down_syndrome_from_Epidemiologic_Point_of_View/links/55f9252308aec948c48d6b62/Down-syndrome-from-Epidemiologic-Point-of-View.pdf
Aldemir, Ö. (2018) The Genetic Aspect of Thalassemia : From Diagnosis to Treatment. In Thalassemia and Other Hemolytic Anemias (InTech,). doi :10.5772/intechopen.76496 Retrieved from https://doi.org/10.5772/intechopen.76496
Aparnna, K. S. & Jose, B. (2014) A Study on the Incidence of Various Genetic Syndromes in Kozhikode District, Kerala, India with special reference to Down Syndrome. 1, 599- 603.
Asim, A., Kumar, A., Muthuswamy, S., Jain, S. & Agarwal, S. (2015) 'down syndrome : An insight of the disease'. Journal of Biomedical Science vol. 22 41. Retrieved from https://doi.org/10.1186/s12929-015-0138-y
Bashyam, M. D. et al. (2004) Molecular genetic analyses of β-thalassemia in South India reveals rare mutations in the β-globin gene. J. Hum. Genet.49, 408-413. Retrieved from https://doi.org/10.1007/s10038-004-0169-9
Black, M. L. et al. (2010) A descriptive profile of β-thalassaemia mutations in India, Pakistan and Sri Lanka. J. Community Genet.1, 149-157. Retrieved from https://doi.org/10.1007/s12687-010-0026-9
Cao, A. & Galanello, R. (2010) Beta-thalassemia. Genetics in Medicine vol. 12 61-76. Retrieved from https://doi.org/10.1097/GIM.0b013e3181cd68ed
Colah, R., Italia, K. & Gorakshakar, A. (2017) Burden of thalassemia in India: The road map for control. Pediatr. Hematol. Oncol. J.2, 79-84. Retrieved from https://doi.org/10.1016/j.phoj.2017.10.002
Eggermann, T. & Schwanitz, G. (2011) Genetics of Down Syndrome. In Genetics and Etiology of Down Syndrome (InTech,). doi :10.5772/17817. Retrieved from https://doi.org/10.5772/17817
Galanello, R. & Origa, R. (2010) Beta-thalassemia. Orphanet Journal of Rare Diseases vol. 5 11. Retrieved from https://doi.org/10.1186/1750-1172-5-11
Ghosh, S. et al. (2011) Epidemiology of down syndrome : New insight into the multidimensional interactions among genetic and environmental risk factors in the oocyte. Am. J. Epidemiol.174, 1009-1016. Retrieved from https://doi.org/10.1093/aje/kwr240
Grow, K., Vashist, M., Abrol, P., Sharma, S. & Yadav, R. (2014) Beta thalassemia in india : Current status and the challenges ahead. Int. J. Pharm. Pharm. Sci.6, 28-33.
Gupta, A. et al. (2003) Molecular genetic testing of β-thalassemia patients of Indian origin and a novel 8-bp deletion mutation at Codons 36/37/38/39. Genet. Test.7, 163-168. Retrieved from https://doi.org/10.1089/109065703322146894
Gupta, A., Shridhar, K. & Dhillon, P. K. (2015) A review of breast cancer awareness among women in India : Cancer literate or awareness deficit? Eur. J. Cancer51, 2058-2066. Retrieved from https://doi.org/10.1016/j.ejca.2015.07.008
Hassan, T. et al. (2016) Β-Thalassemia : Genotypes and Phenotypes. In Epidemiology of Communicable and Non-Communicable Diseases - Attributes of Lifestyle and Nature on Humankind 113-126 (InTech,). doi :10.5772/64644. Retrieved from https://doi.org/10.5772/64644
Kava, M. P., Tullu, M. S., Muranjan, M. N. & Girisha, K. M. (2004) Down syndrome : Clinical profile from India. Arch. Med. Res.35, 31-35. Retrieved from https://doi.org/10.1016/j.arcmed.2003.06.005
Kazemi, M., Salehi, M. & Kheirollahi, M. (2016) Down syndrome : Current status, challenges and future perspective. International Journal of Molecular and Cellular Medicine vol. 5 125-133.
Mohanty, D. et al. (2013) Prevalence of β-thalassemia and other haemoglobinopathies in six cities in India : A multicentre study. J. Community Genet.4, 33-42. Retrieved from https://doi.org/10.1007/s12687-012-0114-0
Panigrahi, I. & Marwaha, R. K. (2007) Mutational spectrum of thalassemias in India [1]. Indian Journal of Human Genetics vol. 13 36-37. Retrieved from https://doi.org/10.4103/0971-6866.32034
Pankaj, G., Avani, K. & Salil, V. (2015) Prevalence of Down Syndrome in Western India: A Cytogenetic Study. Br. J. Med. Med. Res.5, 1255-1259. Retrieved from https://doi.org/10.9734/BJMMR/2015/13648
Plaiasu, V. (2017) Down Syndrome - Genetics and Cardiogenetics. Maedica (Buchar).12, 208-213.
Russell, P. J. (n.d.) iGenetics by Russell. Benjamin Cummings vol. Third Edit.
Shah, P. S. et al. (2017) Mutation analysis of &beta ; -thalassemia in East-Western Indian population : à recent molecular approach. Appl. Clin. Genet.Volume 10, 27-35. Retrieved from https://doi.org/10.2147/TACG.S127531
Sherman, S. L., Allen, E. G., Bean, L. H. & Freeman, S. B. (2007) Epidemiology of Down syndrome. Mental Retardation and Developmental Disabilities Research Reviews vol. 13 221-227. Retrieved from https://doi.org/10.1002/mrdd.20157
Verma, I. C., Lall, M. & Dua Puri, R. (2012) Down Syndrome in India-Diagnosis, Screening, and Prenatal Diagnosis. Clinics in Laboratory Medicine vol. 32 231-248. Retrieved from https://doi.org/10.1016/j.cll.2012.04.010
Wahed, A. & Dasgupta, A. (2015) Hemoglobinopathies and Thalassemias. In Hematology and Coagulation 55-80 (Elsevier,). doi :10.1016/B978-0-12-800241-4.00004-8. Retrieved from https://doi.org/10.1016/B978-0-12-800241-4.00004-8
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2022. All Rights Reserved.